This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Curtain etal1 performed an analysis of the VALIANT (Valsartan in Acute Myocardial Infarction) and PARADISE-MI (Prospective ARNi vs ACE Inhibitor Trial to Determine Superiority in Reducing Heart Failure Events After MI) trials to evaluate whether risk of sudden cardiacarrest (SCA) following acute myocardial infarction (MI) has changed over time.
survival rates from out-of-hospital cardiacarrests fell significantly at the beginning of the COVID-19 pandemic in 2020 and only slightly. This news release contains updated information and data not included in the abstract. Research Highlights: U.S.
Out-of-hospital cardiacarrest survival rates dropped significantly at the onset of the COVID-19 pandemic in 2020 and have continued to remain lower than in the pre-pandemic years of 2015–2019, according to a preliminary study to be presented at the American Heart Association's Scientific Sessions 2024.,
AN evaluation of efficacy amonGst cOmpression only and standard CPR) trial is designed to evaluate whether compression-only cardiopulmonary resuscitation (CPR) by trained laypersons is noninferior to standard CPR in adult out-of-hospital cardiacarrest. Of these, 640 were assigned to intervention and 610 to control.
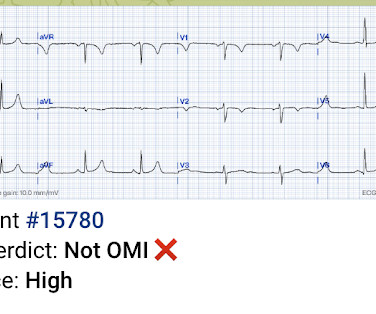
While on telemetry monitoring he suffered cardiacarrest and was resuscitated. What ECG finding may have contributed to (or precipitated) the cardiacarrest? Learning points : Takotsubo can lead to cardiacarrest from ventricular arrhythmia. There are no clear signs of OMI. There is a prolonged QTc.
BackgroundProteinuria is a risk factor for cardiovascular events, but its prognostic value for sudden cardiacarrest (SCA) in young individuals remains unproven. Participants included in the analysis were followedup till December 2020, and Cox proportional hazards model was used to demonstrate the risk of SCA.
BackgroundOutofhospital cardiacarrest (OHCA) with initial shockable rhythm generally has a favorable prognosis. Journal of the American Heart Association, Ahead of Print. However, the prognosis worsens when this rhythm transitions to nonshockable rhythm on hospital arrival.
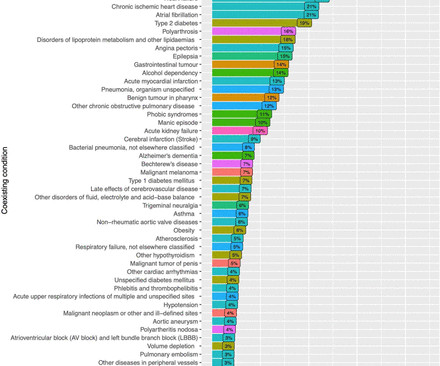
Background Out-of-hospital cardiacarrest (OHCA) has a dismal prognosis with overall survival around 10%. Previously, 80% of sudden cardiacarrest have been attributed to coronary artery disease. We studied comorbidities and discharge diagnoses in OHCA in all of Sweden.
In part due to advances in guideline-directed medical therapy (GDMT) and availability of implantable cardioverter-defibrillators (ICDs), cardiacarrest (CA) rates among patients with heart Failure (HF) decreased in the early 2000s. Relatively little is known about trends in CA associated with HF over the past decade.
A 60-something woman presented after a witnessed cardiacarrest. This is commonly found after epinephrine for cardiacarrest, but could have been pre-existing and a possible contributing factor to cardiacarrest. Final Diagnosis: CardiacArrest due to Torsades from long QT of unknown etiology.
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). As a result — an ICD may need to be considered in selected cases.
Background:Different from the negative impact of COVID-19 pandemic on outcomes after out-of-hospital cardiacarrest (OHCA) collapsed before emergency medical service (EMS) arrival, there was a report suggested that COVID-19 pandemic did not affect outcomes after OHCA witnessed by EMS personnel.
We periodically review this intriguing ECG finding that is best known for its association with hypothermia — but which may also be seen in association with a number of other entities, including acute infarction and cardiacarrest. My Comment addresses a few additional aspects of this phenomenon.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiacarrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. So, your next step is to Trace it down, and Copy it over".
The ECG in Figure-1 — was obtained from a middle-aged man who presented to the ED ( E mergency D epartment ) in cardiacarrest. C ASE C onclusion: As noted above — the middle-aged man in today's case presented to the ED in cardiacarrest. In view of this history — How would YOU interpret the ECG in Figure-1 ?
Blood was drawn , and the patient was promptly placed in a room to be seen — but on entering, the ED physician found her unresponsive in cardiacarrest. Do you see any indication on this ECG of WHY this patient was about to arrest? Is there any indication on this ECG of WHY this patient shortly after had a cardiacarrest?
For technical reasons — P waves are not well visible in this tracing — BUT — the P wave in lead I appears to be larger than the P wave in lead II , which is often a tip-off to LA-LL Reversal ( See My Comment in the November 19, 2020 and the May 24, 2022 posts in Dr. Smith's ECG Blog ).
For more on my systematic approach — Check out My Comment in the May 3, 2020 post ). Smith’s ECG Blog: SQTS is an inherited cardiac channelopathy determined by the presence of symptoms ( syncope, cardiacarrest ) — positive family history — and the ECG finding of an abnormally short QTc interval.
Results From 1 January 2005 to 31 December 2020, 2727/18 988 (14.4%) patients were SMuRF less, with the proportion increasing over time. SMuRF-less patients were more likely to present with cardiacarrest (6.6% Mean age was similar for patients with and without SMuRFs (63 years), and fewer females were SMuRF-less (19.8%
METHODS:This retrospective cohort study analyzed data from 2 academic centers involving patients with intermediate-risk PE from January 2020 to January 2024. The primary outcome was a composite of 30-day mortality, resuscitated cardiacarrest, hemodynamic instability, and 90-day readmission.
This study aims to evaluate the outcomes of chronic opioid therapy on HFpEF patients.Methods:Studying the National Inpatient Sample (2016-2020), we identified adult HFpEF patients using the appropriate ICD-10 codes -after excluding patients with end-stage renal disease (ESRD)- and compared outcomes between chronic opioid users and non-users.
Methods and results 2407 consecutive patients presenting to Harefield Hospital with measured arterial blood gases, from January 2011 to December 2020, were studied to build the training set. 30-day mortality in this group was 17.2%. 1 point, 5–9.9: The validation metrics were excellent with a c-statistic of 0.9,
A total of 406 patients were enrolled at 80 sites between 2016 and 2020. Average age was 64±12 years, 24% were female, 17% had a witnessed out‐of‐hospital cardiacarrest, 27% had in‐hospital cardiacarrest, and 9% were under active cardiopulmonary resuscitation during MCS implantation.
Edited by Bracey, Meyers, Grauer, and Smith A 50-something-year-old female with a history of an unknown personality disorder and alcohol use disorder arrived via EMS following cardiacarrest with return of spontaneous circulation. The described rhythm was an irregular, wide complex rhythm.
Methods and results Among 657 patients enrolled from March 2020 to November 2023, 198 (30.1%) received oxygen therapy (OT), 96 (14.6%) underwent non-invasive ventilation (NIV), and 363 (55.3%) underwent invasive mechanical ventilation (iMV). for the NIV group ( p =0.005), even after excluding patients with cardiacarrest at presentation.
Understanding the association with acute myocarditis (AMC) is crucial for preemptive management strategies and improving patient outcomes.Methods:We identified and compared adults (>18 years) with SID vs. non-SID patients hospitalized with AMC using the National In-patient sample database from 2016-2020.
Data was obtained from the Hospital Corporation of America (HCA) enterprise-wide database from January 2020 to September 2023 using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM).
I suspect this is Type 2 MI due to prolonged severe hypotension from cardiacarrest. Shark Fin morphology has been discussed a number of times on Dr. Smith’s ECG Blog ( For review — See the June 11, 2018 post and the January 24, 2020 post , to name just 2 instances ). 24, 2020 post ( link to that post given above ).
Methods and results This nationwide observational cohort study describes all AMICS patients treated with Impella (ABIOMED, Danvers, MA, USA) and/or VA-ECMO in 2020–2021. Impella patients were older (34% vs. 13% >75 years, p < 0.001) and less frequently presented after an out-of-hospital cardiacarrest (18% vs. 40%, p < 0.001).
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). Regarding AFib with WPW: The very rapid heart rate and at times extremely short R-R intervals put the patient with AFib and WPW at risk of cardiacarrest from VFib.
A man in his 30s with cardiacarrest and STE on the post-ROSC ECG == MY Comment , by K EN G RAUER, MD ( 12/31 /2023 ): == My only hope about today's tragic case — is that the involved providers learn from mistakes made. I include a summarizing Table of ECG Findings in Figure-2 of the ADDENDUM below ).
He has done a lot of great work on cardiacarrest, including as co-author of our study on esmolol in refractory cardiacarrest, and much more with Keith Lurie. This was sent by Guillaume Debaty, from the Grenoble Region of France. See his Google Scholar profile here.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiacarrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). The August 22, 2020 post in Dr. Smith's ECG Blog — which illustrates another case of dynamic ST-T wave changes that resulted from a repolarization variant.
They had had twice the rate of cardiacarrest and twice the in-hospital mortality[1] In another study of patients diagnosed with STEMI, those on dialysis experienced delayed reperfusion and double the mortality.[2] They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
There was 100% proximal LAD occlusion with TIMI 0 flow, and cardiacarrest in the cath lab. The emergency physician asked for stat cardiology consult, bedside echo showed anterior akinesis, and the cath lab was activated – with door-to-cath time of 4 hours. When seen — such ST elevation is typically seen in anterior leads.
I've reproduced this figure from My Comment in the January 6, 2020 post of Dr. Smith's ECG Blog ). See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life.
While hypertension and sinus tachycardia are the most common manifestations — a variety of other tachyarrhythmias ( including VT leading to cardiacarrest ) and acute MI may be seen. Potential cardiovascular effects of acute amphetamine use are multiple.
Series of Prehospital ECGs Showing Reperfusion == MY Comment by K EN G RAUER, MD ( 9/21/2020 ): == I wish those cardiologists who continue to strictly adhere to STEMI millimeter criteria would begin reading Dr. Smith’s ECG Blog. A mysterious case.
It is apparently fortunate that she had a cardiacarrest; otherwise, her ECG would have been ignored. Then they did an MRI: Patient underwent cardiac MRI on 10/4 that showed mildly reduced BiV systolic function. She was defibrillated and resuscitated. Smith: this ECG and clinical presentation is diagnostic of LAD Occlusion.
Physicians initially attributed symptoms to “panic, anxiety or stress” in half of these patients, with women more likely than men to have their symptoms attributed to psychiatric causes (65% vs. 32%; P < 04). == MY Comment by K EN G RAUER, MD ( 9/7/2020 ): == Interesting case with thorough discussion by Dr. Smith on arrhythmia management.
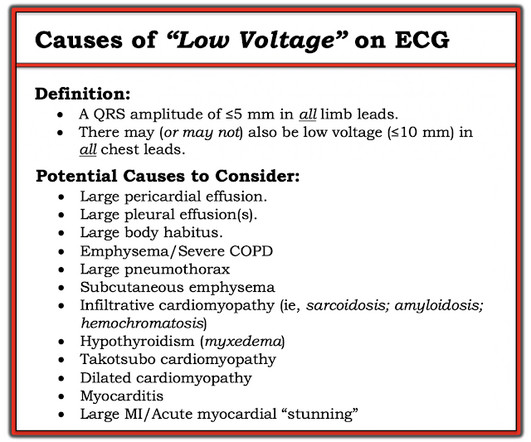
Figure-2: Causes of Low Voltage on ECG ( Figure reproduced from My Comment at the bottom of the page in the November 12, 2020 post in Dr. Smith's ECG Blog ). Figure reproduced from My Comment at the bottom of the page in the September 7, 2020 post in Dr. Smith's ECG Blog ). What is ELECTRICAL ALTERNANS?
Case submitted by Magnus Nossen MD from Norway, written by Pendell Meyers A man in his 50s with no pertinent medical history suffered a witnessed cardiacarrest. 12 minutes later, the patient went back into VFib arrest and underwent another 15 minutes of resuscitation followed by successful defibrillation and sustained ROSC.
A patient had a cardiacarrest with ventricular fibrillation and was successfully defibrillated. Coronary Angiography after CardiacArrest without ST-Segment Elevation. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
Cardiac Troponin Testing in Patients with COVID-19: A Strategy for Testing and Reporting Results. Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. Guo T, Fan Y, Chen M, et al.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content