This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
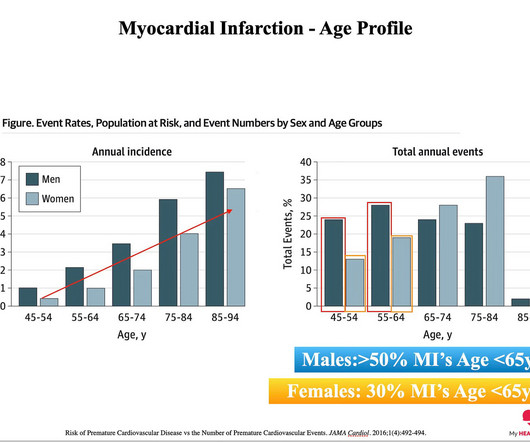
The reason: They were accumulating plaque in their coronary arteries much earlier than their peers. You can’t have a heart attack if you don’t have plaque in your coronary arteries. And plaque in your coronary arteries is the result of exposure to risk factors over time. The answer: Risk Factors. The answer.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. Journal of the American Heart Association, Ahead of Print. Small dense lowdensity lipoprotein cholesterol (sdLDLC) is considered as the most atherogenic lipoprotein.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. See "Mechanisms of acute coronary syndromes related to atherosclerosis".)
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. FFR can be useful.
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
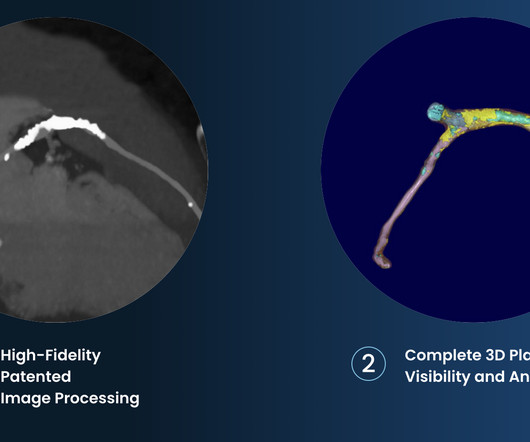
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
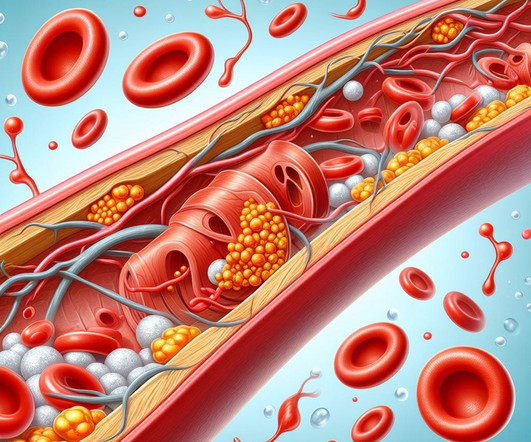
When we say heart disease, what we really mean is plaque in the artery wall. This Is Known As Atherosclerosis. The fundamental cause of atherosclerosis is when a cholesterol particle crosses into the artery wall from the bloodstream, gets stuck, and sets off an inflammatory process 1. No atherosclerosis. No heart attacks.
people from the general population), coronary artery calcium scores (CACS) are higher, indicating more calcification and the presence of atherosclerotic plaques. Calcified plaques are known to be more stable and less prone to rupture and lead to a heart attack. When comparing athletes to control groups (i.e., hours per week).
Heart disease is the presence of plaque or atherosclerosis in the coronary arteries. Over a long enough time horizon, pretty much everyone will develop a significant amount of plaque and have a heart attack. We have very strong evidence to support the idea that the more plaque you have, the greater your risk of a heart attack 1.
However, most adults will start to develop advanced plaque in their coronary arteries early in life. By age 66, more than half of all females will have evidence of advanced plaque in their coronary arteries, as seen on a CT calcium score. Coronary atherosclerosis, as evidenced by an abnormal CAC score, is a measure of advanced plaque.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,6 Until recently atherosclerosis has been thought of as the result of passive lipid accumulation in the vessel wall. 4 In the U.S.
Purpose To evaluate the association between osteoporosis and coronary calcification and coronary plaque burden in patients with atherosclerosis and coronary artery disease (CAD). The coronary artery calcium score (CACS) and total coronary plaque burden were quantified using the Agatston and modified Gensini scores, respectively.
A CT CAC scan can only identify if there is calcified atherosclerosis, where it is and to what extent. A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. A CT CAC scan of 0 indicates no significant amount of calcified atherosclerosis.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronary artery disease (atherosclerosis/plaque) that might rupture and cause a heart attack. And the less plaque you have, the lower the risk of a heart attack. And it’s also WAY more common.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content