This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
age, 54% women, 50% White), finding that a whopping 2M (6.8%) of them had been diagnosed with AFib. AFib rates increased dramatically during the study period, from 4.49% in 2005-2009 to 6.82% in 2015-2019. the researchers estimate that at least 10.55M Americans are currently diagnosed with AFib, representing 4.48% the U.S.
"Based on the results from the admIRE clinical trial, we are confident that this innovation has the promise to deliver significant value and differentiated capabilities, and become an important tool for the treatment of AFib." 2,3 Approximately 1 in 4 adults over the age of 40 are at risk for developing AFib. Epub 2020 Jan 19.
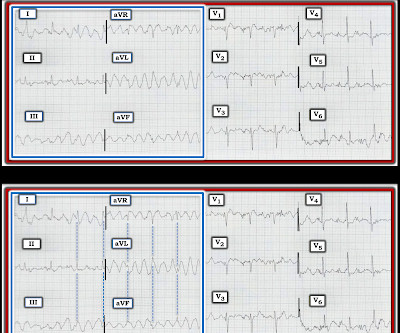
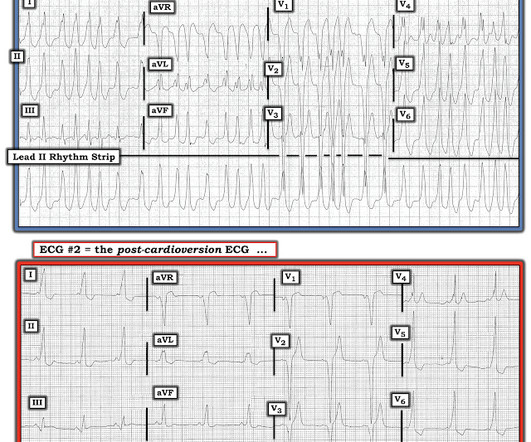
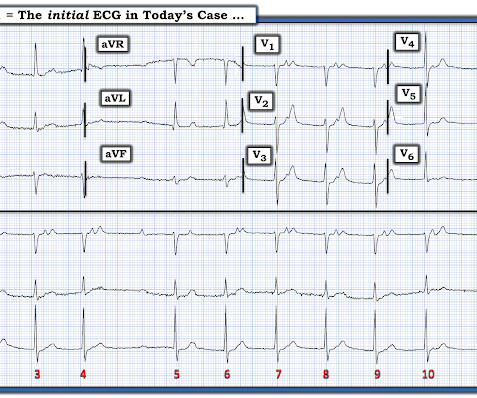
NOTE: The ECGs in today's case are recorded in the Cabrera Format ( See Dr. Grauer Comment in the October 26, 2020 post of Dr. Smith's ECG Blog for review on the Cabrera Format ). KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
The results support the use of workflows to reduce radiation exposure during catheter ablation for the treatment of paroxysmal atrial fibrillation (AFib) while maintaining safety, efficacy, and long-term patient outcomes comparable to traditional procedures.1 2020 June;127(1):4-20. Int J Stroke. 2021 Feb;16(2):217-221.
The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
1] Within the complex umbrella of cardiology care and cardiovascular disease, atrial fibrillation ( AFib ) is the most common arrhythmia diagnosed in clinical practice with projections indicating that the prevalence of AFib could reach 15.9 2020 Aug 11;370:m2724. million people in the United States by 2050 and 17.9
Sci 5[4] 268-270, 2015 ) both highlight a likely association between acute development of ischemic J waves — and high risk of developing malignant ventricular arrhythmias ( My Comment in the September 23, 2020 post ). Baseline artifact is no longer present.
M y I MPRESSION : The rhythm in Figure -1 is almost certain to be very rapid AFib in a patient with WPW. NOTE #2: Surprisingly, it is not uncommon for patients in AFib with WPW to be hemodynamically stable — despite having exceedingly rapid ventricular rates. ECG Blog #284 — Reviews a case similar to today's Very Fast AFib.
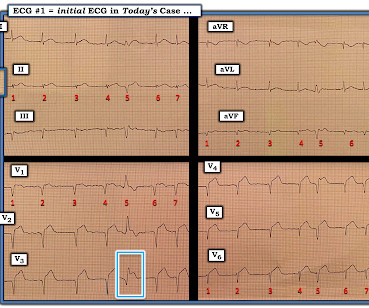
Despite the irregularity of QRS complexes — this rhythm is not AFib — because at least some definite P waves are present ( RED arrows that I added at the bottom of ECG #1 ). Smith has noted — recognition of Shark Fin morphology told us that the seemingly wide and irregular rhythm in Figure-1 was almost certain to be supraventricular!
I was sent the ECG shown in Figure-1 — being told only that providers on the case suspected AFib ( A trial Fib rillation ) with RBBB ( R ight B undle B ranch B lock ) aberrancy. Working through a case of a regular WCT Rhythm in this 80-something woman — See My Comment in the May 5, 2020 post on Dr. Smith’s ECG Blog.
Is longterm endurance-training a risk factor for AFib and AFlutter? == Why is Today's Initial Rhythm AFlutter? Moderate" exercise seems to have a protective effect with reduced risk of AFib — whereas "excessive" exercise has been shown to significantly increase the risk of developing AFib, especially as adults age.
As we often emphasize ( See My Comment in the May 5, 2020 post of Dr. Smith's ECG Blog ) — Statistically (ie, even before we look at the ECG itself ) — at least 80% of all regular WCT rhythms without clear sign of P waves will turn out to be VT ( V entricular T achycardia ). I'd add the following thoughts to Dr. Smith's discussion.
== MY Comment by K EN G RAUER, MD ( 3/12/2020 ): == A young adult presented to the ED with the “heart awareness” and the ECG shown in Figure-1 — but with no more than slight shortness of breath. Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response.
AFib Facts and Impacts Atrial fibrillation is the most common cardiac arrhythmia, affecting 2% of individuals worldwide. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). doi:10.1093/europace/euae043. Eur Heart J.
This defines the rhythm as AFib ( A trial F ibrillation ) , here with a controlled ventricular response ( ie, overall heart rate between ~70-to-100/minute ). Recognizing hyperacute T waves — patterns of leads — an OMI ( though not a STEMI ) — See My Comment at the bottom of the page in the November 8, 2020 post on Dr. Smith's ECG Blog.
HCM is an "umbrella term" applied to the presence of LVH in the absence of "abnormal cardiac loading conditions" ( Hughes et al — JAHA 9:e015294, 2020 ). WPW Cardiac arrhythmias ( including AFib ). Tall R wave in lead V1 and/or early transition in the chest leads ( reflecting increased "septal" forces ).
As a result, in order to differentiate MAT from the much more commonly encountered irregularly irregular rhythm ( which is AFib ) — we need to be certain we are seeing multiple different P wave morphologies that are constantly changing. Clinically , the importance of recognizing MAT — is that treatment is different than the treatment of AFib.
The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
For more on Giant T waves — See My Comment at the bottom of the page in the June 22, 2020 and September 19, 2022 posts in Dr. Smith's ECG Blog ). Types of HCM: As per Hughes et al ( JAHA 9:e015294, 2020 ) — HCM is an "umbrella term" applied to the presence of LVH in the absence of "abnormal cardiac loading conditions".
The rhythm is rapid AFib. These are the "Take-Home" Lessons from today's tracing: As per Dr. Smith — Rapid AFib may sometimes simulate acute posterior OMI. This anterior ST depression often resolves ( or at least greatly decreases ) when AFib is controlled and the heart rate slows. The February 11, 2020 post ( LA-RA reversal ).
See this terrible case: Computer often fails to diagnose atrial fibrillation in ventricular paced rhythm, and that can be catastrophic == MY Comment , by K EN G RAUER, MD ( 1/22/2020 ): == Our THANKS to Dr. Smith for presenting this extremely interesting case. Clinically What has happened in the interim?
The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
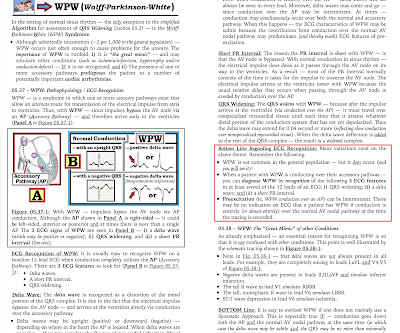
Patient was referred to electrophysiologic testing due to suspicion of afib and WPW. During electrophysiologic testing AVRT was induced, which degenerated to afib with ortho and antidromic conduction. Despite the near regularity in places — the reasons I immediately thought of WPW with very rapid AFib were i ) As per per Drs.
Time Window for Reperfusion; Acuteness on the ECG) == MY Comment by K EN G RAUER, MD ( 8/13/2020 ): == This is a challenging case — which is made all the more difficult by suboptimal quality of the initial 12-lead ECG — and lack of additional simultaneously-recorded leads for the arrhythmia tracings. Would you give Thrombolytics?
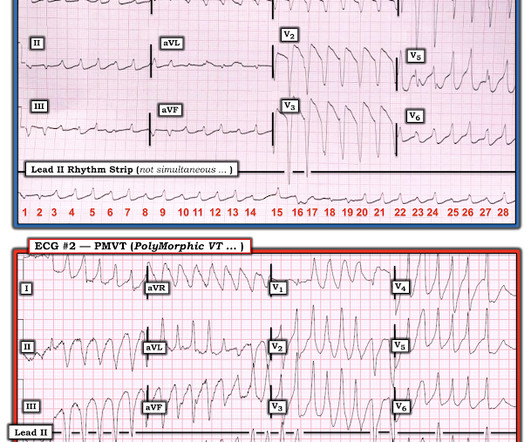
== MY Comment by K EN G RAUER, MD ( 6/1 /2020 ): == YOU are asked to interpret the ECG shown in Figure-1. MY THOUGHTS on ECG #1: My initial impression on looking at the ECG in Figure-1 — was that the rhythm was either rapid AFib in a patient with WPW — or — PMVT ( P oly M orphic VT ). Unfortunately, no history is available to assist.
For more on my systematic approach — Check out My Comment in the May 3, 2020 post ). Assuming the patient did not have hypercalcemia and there was no history of cardiac arrest, unexplained syncope or AFib at an early age — cardiac risk from a “short” QTc is clearly less than for patients with frank SQTC.
MY Thoughts on Today's ECG: As per Dr. Smith — the rhythm in ECG #1 appears to be AFib with a controlled ventricular response ( ie, irregularly irregular without clear sign of P waves ). Figure-1: The initial ECG in today's case. ( To improve visualization — I've digitized the original ECG using PMcardio ). What else?
I have periodically called attention to examples of the Ashman phenomenon as they occur in Dr. Smith's ECG Blog ( See My Comments in the January 5, 2020 post — the June 17, 2020 post — and the March 30, 2023 post , among others ).
I see the following: Although there is no long lead rhythm strip — we can see that the rhythm is AFib with a controlled ventricular response ( ie, irregularly irregular rhythm without P waves — and with a heart rate between ~70-110/minute ). Regarding Intervals: There is no PR interval ( since the rhythm is AFib ).
ECG Blog #71 — Regarding the Ashman Phenomenon with AFib. These cases provide insight to assessment for MAT: The January 5, 2020 post in Dr. Smith’s ECG Blog — for an example of MAT. ECG Blog #70 — Reviews the A shman P henomenon ( re aberrant conduction ). I link to 2 additional illustrative Cases taken from Dr. Smith’s ECG Blog.
Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular. P utting I t A ll T ogether : — The Rhythm in Figure-1 What we have just described is the following: A regular WCT ( = W ide- C omplex T achycardia ) at a rate very close to 300/minute — without clear sign of atrial activity.
The patient also has a history of AFib and HFmrEF ( = H eart F ailure with M inimally- R educed E jection F raction ). The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). This patient presented to the ED “after a couple of days of chest discomfort”.
The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog. What is certain — is the continued marked ST depression in the mid-chest leads, consistent with an ongoing, extensive infarction in this patient with severe symptoms and hypotension. =
of all cases, and 62% of Veritas® misdiagnoses). == MY Comment , by K EN G RAUER, MD ( 1/5/2020 ): == This case illustrates a number of important teaching points. AFib is the irregularly irregular rhythm that is most commonly confused with MAT — and , AFib is much, much, much more common than true MAT. GET a 12-lead!
The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
Resuscitation was initiated and this ECG was obtained: Likely AFib (irregularly irregular) with bradycardia. Consider thrombolytics for OMI when PCI is not an option. == MY Comment by K EN G RAUER, MD ( 1/19/2020 ): == There is a LOT to talk about regarding the series of tracings in this unfortunate case.
and if not — Is the rhythm “irregularly irregular”, as in AFib — or is there a pattern of “regular" irregularity in the form of group beating ? ). What is the R ate? looking both at the atrial and ventricular rates IF these are different ). Is the rhythm R egular? ( If P waves are present — Are P waves R elated to neighboring QRS complexes?
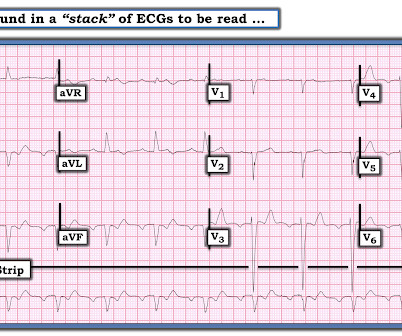
Diagnosis : Extremely slow Atrial flutter == MY Comment , by K EN G RAUER, MD ( 11/15/2020 ): == Some of the most interesting ECG cases I have seen have been picked up “reading through a stack of ECGs” — in the same manner that Dr. Smith picked up today’s case. Atrial arrhythmias ( especially AFib or AFlutter ). Prolonged QTc interval.
Is This a Simple Right Bundle Branch Block? == MY Comment , by K EN G RAUER, MD ( 1/26/2020 ): == Dr. Smiths ECG Blog has presented too-numerous-to-count cases of hyperkalemia ( See My Comment in the 12/11/2018 post there are many others! ). Is this just right bundle branch block?
Assuming there was no history of cardiac arrest, unexplained syncope or AFib at an early age — cardiac risk from a “short” QTc is clearly less than for patients with frank SQTC.
Figure-4: I’ve postulated a laddergram for ECG #3 in Today’s Case ( For more on the use of laddergrams — See My Comment in the February 20, 2020 post ). That said — ATach can not be ruled out until EP study is done. Our THANKS to Dr. Smith for presenting this case!
Note: The ECG in Figure-1 was initially recorded using the Cabrera Format ( See Comment by Dr. Grauer at the bottom of the page in the October 26, 2020 post for review of the Cabrera Format ). The AFib had been well controlled on Flecainide for many years. Facilitating conversion of AFib to AFlutter as another proarrhythmic effect.
The April 6, 2023 post — excessive baseline artifact misdiagnosed as AFib ( instead of sinus rhythm with AV Wenckebach — as in Figure-4 in this post ). The November 10, 2020 post — for PTA. The October 17, 2020 post — for a 70-year old woman with " Artifactual VT ". The March 17, 2023 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content