This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
Even with tachycardia and a paced QRS duration of ~0.16 2 Quick Approximations that I Use: As I discuss in My Comment in the March 19, 2019 post in Dr. Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol. As per the text under the ECG in Figure-1 you only need to remember 3 values ( ie, 1.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? However, until such time that we know for certain — I think it best to simply describe what we see: PEARL # 1: Realize that for any tachycardia — there are 6 Parameters that need to be assessed. Are flutter waves hidden within the QRS and T waves? s in Figure-2 ).
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrial flutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Or are they due to ventricular tachycardia (VT). Within about an hour, he spontaneously converted to sinus rhythm: == My Comment by K EN G RAUER, MD ( 4/23/2019 ): == Interesting rhythm — in which the tachycardia alternates from a wide to narrow QRS complex. There are no P-waves. Sinus P waves are absent.
RBBB is no longer seen after conversion to sinus rhythm — which supports our suspicion that the intermittent RBBB conduction seen every-other-beat during the tachycardia ( in Figure-1 ) was rate-related. Note that QRS morphology after conversion to sinus rhythm is very similar to QRS morphology of odd-numbered beats during the tachycardia.
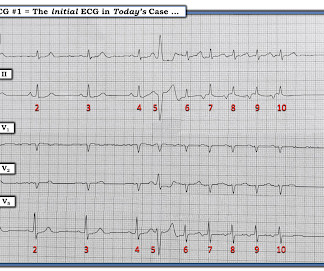
The rhythm is regular — at a rate just over 100/minute = sinus tachycardia ( ie, the R-R interval is just under 3 large boxes in duration ). Continuing with assessment of ECG #1 in Figure-2: The rhythm is sinus tachycardia at ~110/minute. Figure-2: I've labeled the initial ECG. The QRS complex is obviously wide.
Multifocal Atrial Tachycardia 2. IJC Heart and Vasculature 25(2019). P EARL # 4 — In “real life” — there is often NO distinct “cut-off” for differentiating between sinus tachycardia with multiple different-looking PACs vs MAT. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. More cases on WPW with atrial fibrillation : A young man with another episode of tachycardia. What is it? And why give adenosine in sinus rhythm? 3) Buttner, R.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
You are shown the ECG in Figure-1 — told only that the patient had a “continuous" tachycardia. PEARL # 4: This less common form of "fast-slow" AVNRT that is illustrated in Figure-3 — has also been known as an "incessant" tachycardia. ECG Blog #138 — AFlutter vs Atrial Tachycardia. What is the differential diagnosis?
With normal EF the tachycardia is not compensatory. And the patient has sinus tachycardia. ( On arrival patient was slightly tachycardic. HR about 90-100/min. Other vital signs normal. Hand held echo showed overall ejection fraction being normal. ACS then becomes less likely. Final diagnosis was myocarditis. at ~100/minute ).
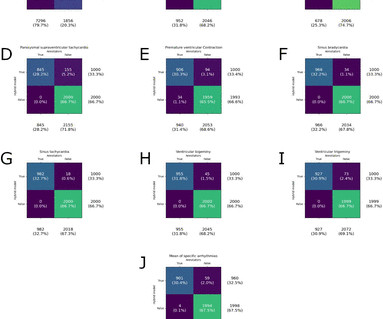
Performance was best for pause (F 1 Score, 99%) and worst for paroxysmal supraventricular tachycardia (F 1 Score, 92%). for paroxysmal supraventricular tachycardia. We calculated classifier statistics for each arrhythmia, all arrhythmias and strips where the model identified normal sinus rhythm. for pause to 7.2%
I focus my thoughts on a qualitative approach to these 3 pre-hospital ECGs — all obtained from patients presenting with acute CP ( C hest P ain ). == ECG #1 — from a 70-ish year old Woman with acute CP and Dyspnea The rhythm is sinus tachycardia at a surprisingly rapid rate of ~115/minute.
The importance of determining whether the QRS complex of a tachycardia is wide or narrow — is that IF the QRS is narrow in all 12 leads, then the rhythm is supraventricular ( and we have therefore ruled out the possibility of VT = Ventricular Tachycardia ). PEARL # 1: Remember the saying, “12 leads are better than one”.
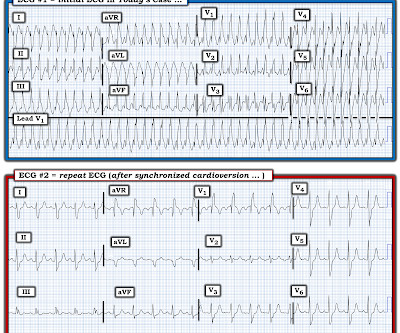
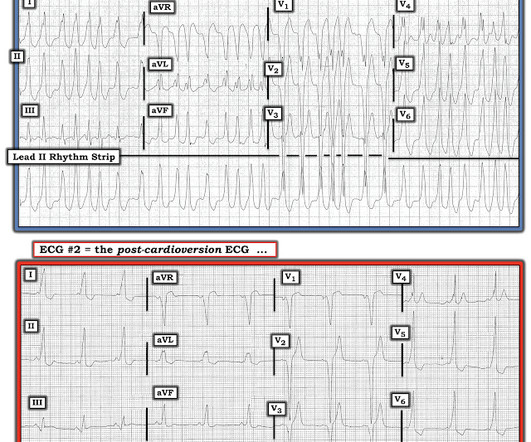
IF today’s rhythm was an SVT — a rate of 250-260/minute is clearly too fast to be sinus tachycardia. Case CONCLUSION: The repeat ECG in Figure-3 shows conversion of the rhythm in ECG #1 to sinus tachycardia ( restoration of upright sinus P waves in lead II — at a rate of ~110/minute ).
== MY Comment by K EN G RAUER, MD ( 11/12/2019 ): == My appreciation to Kenneth Khoo for this case. M y A pproach to this R hythm : I reviewed the basics for rhythm interpretation in the October 16, 2019 Case from Dr. Smith’s ECG Blog. This patient was hemodynamically stable. What do YOU think the rhythm is?
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
These 5 parameters are easily remembered by the saying, “Watch your Ps, Qs & the 3 Rs” ( See My Comment in the October 16, 2019 post ). DDx of Polymorphic wide tachycardia: 1. DDx of irregularly irregular wide complex tachycardia : 1. Wide complex tachycardia 2. polymorphic VT or 2. atrial fib with WPW.
By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrial flutter or fibrillation, MAT, AVRT/AVNRT, among others. Why Isn’t this a Run of Atrial Tachycardia? — ECG Blog #138 — AFlutter vs Atrial Tachycardia. ECG Blog #40 — Another regular SVT that turned out to be AFlutter.
Here was the ECG: There is sinus tachycardia. This was sent by a reader. A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. and K was normal. This is "Shark Fin" morphology. I did recognize the S hark F in m orphology of dramatic ST elevation.
Methods This monocentric, prospective, observational study included consecutive patients with unexplained syncope undergoing ILR implantation between October 2007 and 2019. Overall arrhythmogenic diagnostic yield counted 27% (73% sick sinus syndrome, 20% atrioventricular block, and 7% ventricular tachycardia).
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chest pain and normal vitals except tachycardia at about 115 bpm. As Ken says below, tachycardia is not common in OMI and distorts the ST segment, so managing the tachycardia and repeating the ECG is a good strategy.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( How would YOU interpret this tracing? How to manage the patient?
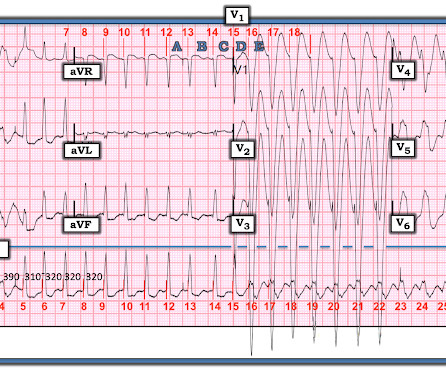
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Tachycardia and ST Elevation. Christmas Eve Special Gift!! Is this inferor STEMI?
There is sinus tachycardia at ~100/minute. As often emphasized by Dr. Smith — sinus tachycardia is not a common finding with acute OMI unless something else is going on (ie, cardiogenic shock ). In today's case — the sinus tachycardia may have been a harbinger of this patient's ultimate demise.
Am J Med 2019, 132(5):622-630. Now there is a paper published in 2019 that proves the point beyond doubt, though makes it clear that this pattern is associated with very high mortality. American Journal of Medicine 132(5):622-630; May 2019. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity.
Tachycardia (or nearly) 2. Tachycardia, = 1.8. Finally , they found these independent predictors of PE: Note that tachycardia only has an Odds ratio of 1.8. Tachycardia is unusual in ACS unless there is cardiogenic shock or a second simultaneous pathology. Some providers were worried about ACS because of this ECG.
See this case, where a patient with BTWI morphology and dramatic EKG changes within minutes is diagnosed with myocarditis: [link] com/2019/07/what-does-this- ecg-with-significant-st.html EKG 3 also has a saddleback morphology in V2, which is only rarely due to OMI. Still, such dramatic changes cannot be overlooked. It was stented.
The September 30, 2019 post in Dr. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia. These cases provide insight to assessment for MAT: The January 5, 2020 post in Dr. Smith’s ECG Blog — for an example of MAT.
Don't miss case 4 at the bottom. == Comment by K EN G RAUER, MD ( 7/1/2019 ): == The ECG diagnosis of BBB ( B undle B ranch B lock ) has long been a source of potential confusion for many interpreters. The rhythm is sinus tachycardia at ~105/minute. The rhythm is sinus tachycardia at ~115/minute.
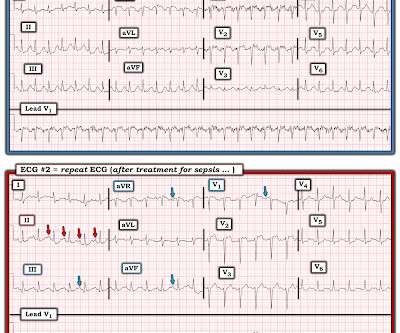
ANSWER: Treatment of the exceedingly rapid (ie, 1:1 AV conduction ) pattern of AFlutter seen in ECG #1 — resulted in considerable slowing of the rhythm, as seen in ECG #2 : The rhythm in ECG #2 — is a regular tachycardia at a rate just under 150/minute ( ie, about half as fast as the rhythm in ECG #1 ). ECG Blog #287 — More on AFlutter.
(acute MI, not pericarditis) You Diagnose Pericarditis at your Peril (at the Patient's Peril!) --Acute MI misdiagnosed as pericarditis. == MY Comment by K EN G RAUER, MD ( 12/13/2019 ): == I LOVE this post — as it explores the important decision-making process associated with the ED diagnosis of a cute P ericarditis.
Jimenez and Ali co-founded AccurKardia in 2019 with a vision for unlocking the value of the ECG signal, and the company currently markets one of the few FDA-cleared solutions for automated ECG interpretation and arrhythmia detection.
No more abnormal U-waves == MY Comment, by K EN G RAUER, MD ( 11/18/2019 ): == LOTS of great points regarding use of the ECG in association with electrolyte abnormalities. Y OU s hould h ave n oted the following additional ECG findings in ECG #1 : There is sinus tachycardia at ~100/minute in ECG #1. second ).
I learned more about the history: 30-something African American with 5-7days of sharp R-sided shoulder/scapula/chest discomfort, presented with sinus tachycardia. Definitive diagnosis is by MRI. This history of a week of constant chest pain is also much more suggestive of myocarditis. OMI it is very unlikely with a week of constant pain.
C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. ECG findings in this case are subtle — and worthy of repetition. CLICK HERE — for my detailed discussion of this subject ). A majority of patients with MAT have longstanding pulmonary disease.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content