This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The past five years have yielded impressive advancements in fully absorbable metal stent technology. Nowhere is the need for fully absorbable metal stents greater than in patients experiencing vascular anomalies associated with congenital heart disease (CHD).
(Gore) announced recent FDA approval of a lower profile GORE VIABAHN VBX Balloon Expandable Endoprosthesis ( VBX Stent Graft ). 1-3 "Our team is pleased to be the first commercial implanter of the new lower profile VBX Stent Graft," said Darren Schneider , M.D., No changes to the stent design were made to achieve the lower profile.
BACKGROUND:Carotid artery stenting (CAS) is an alternative treatment for patients with carotid artery stenosis who are not eligible for carotid endarterectomy. Stroke, Ahead of Print. Dual antiplatelet therapy (DAPT) after CAS aims to prevent ischemic stroke. However, its optimal duration remains unclear.
IntroductionCurrent literature suggests a benefit in functional outcomes and reperfusion rates when carotid artery stenting (CAS) and mechanical thrombectomy (MT) are performed emergently. Stent placement was feasible in all cases. Dual antiplatelet therapy with aspirin and clopidogrel was used in 15 patients before stenting.
To our knowledge, no studies have directly compared the right and left TRA for carotid artery stenting (CAS). The right TRA was performed as a first-line approach from 2019 to 2021, with the left TRA being used thereafter.
Background:Stopping aspirin within 1 month after implantation of a drug-eluting stent (DES) for ticagrelor monotherapy has not been exclusively evaluated for patients with acute coronary syndrome (ACS). Circulation, Ahead of Print. versus 3.4%; HR, 0.35 [95% CI, 0.20–0.61];P<0.001).Conclusions:This 0.61];P<0.001).Conclusions:This
Background:Hyperperfusion phenomenon (HPP) constitutes a significant risk factor for adverse outcomes following carotid artery stenting (CAS). Stroke, Volume 56, Issue Suppl_1 , Page ATP178-ATP178, February 1, 2025. Currently, the sole method for evaluating the risk of HPP post-CAS is the invasive acetazolamide (ACZ) challenge test.
It can provide intraluminal fly-through and clipping-plane views which help endovascular assessment of stents, aneurysms, vessel wall irregularities and calcification. 2019 Nov;14(6):1046-1057. 2019 Nov;14(6):1046-1057. Epub 2019 Sep 4. Reference Kang SL, Armstrong A, Krings G, Benson L. Congenit Heart Dis. Cardiol Young.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
IntroductionThe 2015 American Heart Association Guidelines recommended mechanical thrombectomy with stent‐retriever devices. We analyze the national trends in mechanical thrombectomy use and outcomes for stroke five years after publication of the US guideline update.MethodsWe analyzed the National Inpatient Sample from 2012‐2019.
Methods We retrospectively reviewed children with congenital heart diseases (CHDs) who received trans-axillary arterial catheterizations between January 2019 and February 2023. Overall, 27/36 procedures were interventional, including 6 aortic valvuloplasties, 6 balloon angioplasties, and 15 stenting procedures. months (IQR, 0.3–5.4),
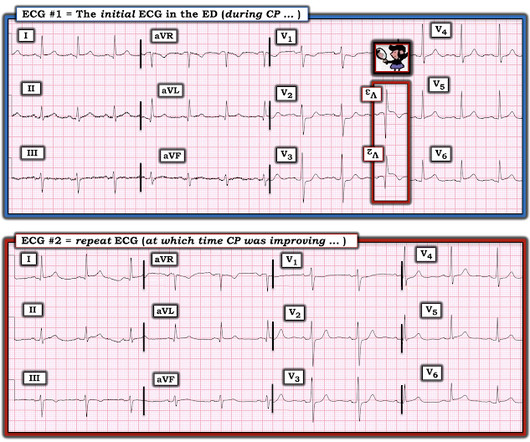
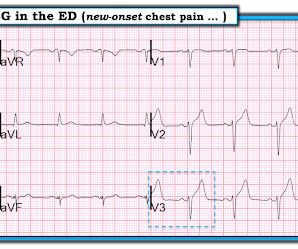
This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. In a word — Patient #2 was lucky to have his ECG interpreted by the Queen Of Hearts.
At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. In fact, this patient had an extensive hx of prior MIs. The ECG (ECG#2) on file that was given you was obtained three months prior. Troponin I peaked at 18.323ng/L.
The studies were classified in 3 periods by publication date: Period 1: before 2015, pre-stent retriever; Period 2: 2015-2019, early thrombectomy era; and Period 3: 2020-2024, recent period.Results:Of 2693 references, 21 trials met inclusion criteria, 3 in Period 1, 10 in Period 2, 8 in Period 3.
first reported 3 patients with vertebral webs diagnosed by DSA and having MRI show ischemic strokes in the vascular territory were treated with endovascular stenting and had no recurrence of an ischemic event (4). Lenck et al.
7 The use of antiplatelet agents to prevent stent thrombosis, moderate- to high-dose statin therapy after acute coronary syndromes, or antihypertensive agents in asymptomatic patients may all be perceived by patients as not providing benefit because they may not feel the effects.8
The primary efficacy objective was to demonstrate superiority of PPA to reduce the primary efficacy end point of all-cause death, nonfatal myocardial infarction, nonfatal stroke, stent thrombosis (definite), or urgent revascularization (any vessel) within 30 days. to 1.57]).
Two adjunctive modifications of CE ‐ balloon remodeling techniques (BRT) and stent‐assisted coiling (SAC) ‐ have been utilized to facilitate occlusion of BTAs of variable anatomies/morphologies, sizes, and rupture status. Stents approved by FDA after 2014 (used in 13 cases) had a greater rate of retreatment (46.2% vs. 10.7%).
We excluded patients who had a clear contraindication to Eptifibatide, received a stent, or if the luminal stenosis was related to reactive vasospasm and any cases with TICI 0, 1, or TICI 3 scores.Results:Our sample size was 60 (51.7% female, mean age 63.9).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. It was stented. He wrote most of it and I (Smith) edited. Still, such dramatic changes cannot be overlooked. V2 has some features of type 2 Brugada phenocopy. This was a large OMI.
Here we showed the efficacy and safety of PCSK9 inhibitor injection immediately prior to mechanical thrombectomy for these patients.MethodsThe subjects were stroke patients who underwent mechanical thrombectomy at Inha University Hospital from April 2019 to March 2023. vs 53.4%, p = 0.04).
IntroductionTo provide our single‐institution experience and outcome data with the WEB device in 51 patients treated for ruptured and unruptured intracranial aneurysms.MethodsOcclusion rates in a cohort of 51 patients treated with WEB were collected at time of procedure and at last follow‐up between the years 2019 and 2021.
One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Angiogram: Severe diffuse left main disease, up to 80% at the ostial left main. Post cath ECG: Normal or near normal Peak troponin I was 15 ng/mL.
One stent was deployed with restorative TIMI-0 flow. However, when the Troponin I returned 8.4 ng/mL during the night – in the presence of unmitigated pain – cardiology decided to take him to the Cath Lab. The red arrow shows a 90% LAD occlusion at the D1 branch. it has been subsequently deemed a STEMI-equivalent.
Clinical outcome was treatment‐related visual complications.ResultsA total of 60 patients treated at our tertiary center between January 2017 and November 2019 were reviewed. Imaging outcomes were aneurysm occlusion and OA patency at 1‐year, determined by Digital Subtraction Angiography (DSA) or MRA. 4 patients were lost to follow up.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. the most commonly overlooked arrhythmia ( See My Comment at the bottom of the page in the May 1, 2023 — and the November 12, 2019 post , among others ). The last echocardiography 12 months ago showed HFmrEF.
It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. When I didn’t — I went back to the August 9, 2019 Post that Dr. Smith references in his comments above. I have summarized the major points from Dr. Smith’s 8/9/2019 post in Figure-1. OM1 is occluded and OM2 has 60% stenosis.
5 ICSS‐ MRI study (International Carotid Stenting Study Magnetic Resonance Imaging Study), indicated that patients with periprocedural hemodynamic depression had decreased cerebral blood flow and increased the risk of new lesions in imaging.6 This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7
LAD and D1 were stented, but flow unfortunately could not be well restored despite efforts (they list the post intervention TIMI flow still as 0). We wrote this Editorial in the Journal of Electrocardiology in 2019. Serial tracings following stent placement confirmed the large extent of myocardial injury.
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis? Compare with an old ECG.
Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented. The nearest PCI center was activated but ultimately denied by Cardiology. Chapter 22: Electrolytes, Temperature, Central Nervous System Disease, and Miscellaneous Effects. Elsevier-Saunders: Philadelphia, PA. [5]. McCance, K.
They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result. Ongoing ischemia (by symptoms, ECG, or troponin) despite maximal medical management is an indication for emergent cath lab activation. == MY Comment by K EN G RAUER, MD ( 8/15/2019 ): == Once again, the w rong q uestion was a sked in this case.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al. J Electrocardiol 2019 6. -- Amsterdam EA, Wenger NK, Brindis RG, et al. Ischemic ST depression maximal in V1-V4 (vs.
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Medicine (Baltimore).
A mid-LAD culprit lesion was identified and stented. Cardiology felt her chest pain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. References Naidu, S. American College of Cardiology.
100% proximal LAD successfully stented. I recognized this as a STEMI immediately and I was only able to do so solely because of your blog." == Comment by K EN G RAUER, MD ( 8/18/2019 ): == Our thanks to Dr. "Cardiology agreed to take the pt to the lab but thought it would likely be negative. Defibrillated out of v fib in the cath lab.
It was stented with good results. Formal Echo next morning: The estimated left ventricular ejection fraction is 44%. Regional wall motion abnormality-mid to basal infero-lateral. Regional wall motion abnormality-basal anterolateral.
Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. See this: Classic Evolution of Wellens' T-waves over 26 hours And a bit of further evolution here. The estimated left ventricular ejection fraction is 61 %.
The culprit lesion was opened and stented. For more on this mirror-image opposite ST-T wave relation in leads III vs aVL — See My Comment in the March 8, 2019 and August 9, 2018 posts in Dr. Smith's ECG Blog ). The QoH now recognizes the OMI with mid confidence. Below is the post -PCI electrocardiogram.
It was stented. == MY Comment by K EN G RAUER, MD ( 9/27/2019 ): == As suggested by the title of this Blog post — confirmation of the diagnosis in this case was made not by ECG — but instead by chest aorta CT !
Here is the post stent ECG: This is probably the amount of ST elevation (zero) that this patient has at baseline. At angiogram with a rapid door to balloon time: Culprit is 100% occlusion of the LAD Mid segment. Note the beginning of Wellens' (reperfusion T-waves) in V3-V6.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
They were stented. We wrote this Editorial in the Journal of Electrocardiology in 2019. [link] Unbeknownst to us at the time, there was an old ECG for comparison from 3.5 years prior which I only found a day later: This is a truly normal ECG, with normal sized T-waves and normal S-waves in V2 and V3. The peak troponin was 1863 ng/L.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content