This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result. Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
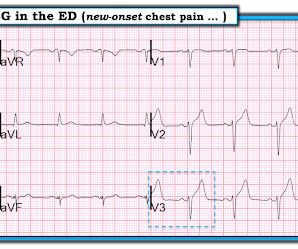
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. It was stented. This was a large OMI.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Unfortunately, we do not have those images for review, but the operators described a ruptured LAD plaque and they stented this area, which ensures the stability of the plaque. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
One stent was deployed with restorative TIMI-0 flow. link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….) it has been subsequently deemed a STEMI-equivalent.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
The primary efficacy objective was to demonstrate superiority of PPA to reduce the primary efficacy end point of all-cause death, nonfatal myocardial infarction, nonfatal stroke, stent thrombosis (definite), or urgent revascularization (any vessel) within 30 days. to 1.57]).
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Bedside echo revealed anteroseptal wall motion abnormality at which point I activated a code STEMI. 100% proximal LAD successfully stented. mm in men over age 40.
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. The cath lab was now activated.
One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Angiogram: Severe diffuse left main disease, up to 80% at the ostial left main. Post cath ECG: Normal or near normal Peak troponin I was 15 ng/mL. Is this OMI?
Computer interpretation: SINUS RHYTHM NON-DIAGNOSTIC ANTEROLATERAL ST ELEVATION BORDERLINE ECG The overreading cardiologist confirmed the computer interpretation (did not diagnose OMI or STEMI). Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. A mid-LAD culprit lesion was identified and stented. Smith comment : V5 and V6 are excessively discordant!!!! References Naidu, S.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. He was successfully stented.
It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. When I didn’t — I went back to the August 9, 2019 Post that Dr. Smith references in his comments above. I have summarized the major points from Dr. Smith’s 8/9/2019 post in Figure-1. OM1 is occluded and OM2 has 60% stenosis.
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? Learning Points: Not all OMI will present as STEMIs.
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented.
They were stented. We wrote this Editorial in the Journal of Electrocardiology in 2019. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion.
I describe and illustrate in detail my approach to incorporating these criteria in My Comment at the bottom of the December 16, 2019 post in Dr. Smiths ECG Blog. However, the cath lab activation was cancelled by the on-call interventionalist who felt the diagnosis of acute STEMI could not be made because of the LBBB.
There is STE that does not meet STEMI criteria in V1-V6. Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. This was mistaken by the treating physicians for ST depression initially. Precordial leads: What do you think? This is diagnostic of LAD OMI.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronary artery disease with a near-occlusive culprit lesion in the RCA, possibly reperfused. To our knowledge, the patient did well.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
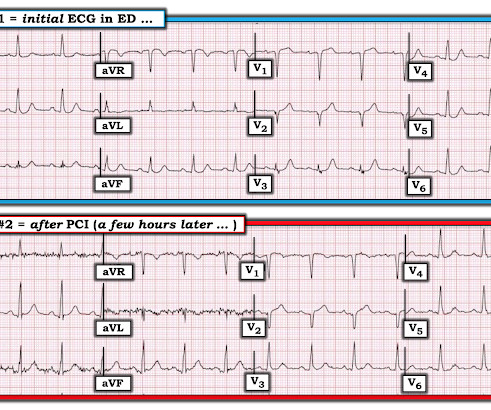
The culprit lesion was opened and stented. For more on this mirror-image opposite ST-T wave relation in leads III vs aVL — See My Comment in the March 8, 2019 and August 9, 2018 posts in Dr. Smith's ECG Blog ). The QoH now recognizes the OMI with mid confidence. Below is the post -PCI electrocardiogram.
The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. 2019 Apr;21(5):253-258. You may see a filling defect in distal LAD, most probably due to an embolization from proximal lesion. Also note that LAD does not extensively wrap-around apex and supply inferior wall. Anatol J Cardiol.
distal stent patent. PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI.
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." The ECG remains positive for STEMI by GE. The true AV groove LCx was "jailed" by the stent and appears occluded in the post PCI image. The emergency physician consulted cardiology.
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. Written by Pendell Meyers An adult man presented with acute chest pain.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent"). It was treated with a drug eluting stent. He just graduated from college. He has no medical training, but he has read this blog for years. Lucky Hans.
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. 5 years later ( now in 2025 ) the problem remains.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. It was opened and stented. The August 26, 2019 post — baseline artifact.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content