This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
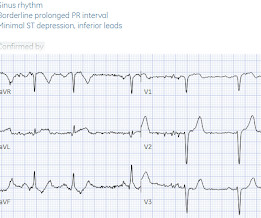
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
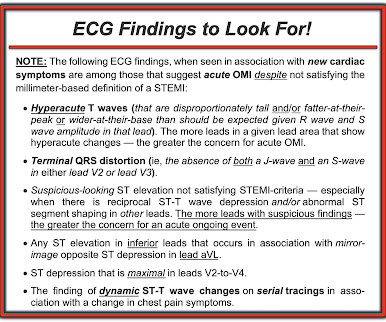
Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG. For my clarifying Figure illustrating T-QRS-D ( 2nd bullet ) — See My Comment at the bottom of the page in Dr. Smith’s November 14, 2019 post. = ECG Blog #205 = The Systematic Approach I favor.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
The post EM Quick Hits 4 Acetaminophen Overdose & Warfarin Interaction, Dental Infections, MTP RABT Score, Statins for STEMI, Cricothyrotomy Tips appeared first on Emergency Medicine Cases.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute. What is M INOCA?
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
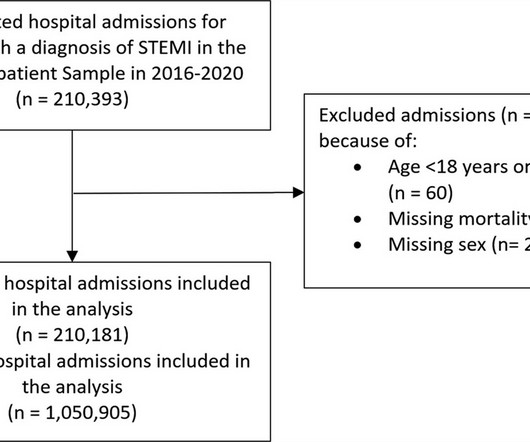
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% for patients admitted in 2016–2019 period. reduction in admissions in 2020.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The January 9, 2019 post in Dr. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ).
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. A millimeter definition of acute STEMI should not be needed to justify the need for prompt cardiac catheterization.
This was a machine read STEMI positive OMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury. What would you guess is the culprit artery?
Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients. All patients with STEMI underwent CPFD-caIMR and MVO assessment.
Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre. Quality initiatives aimed at improving the care of this vulnerable, yet understudied population are needed.
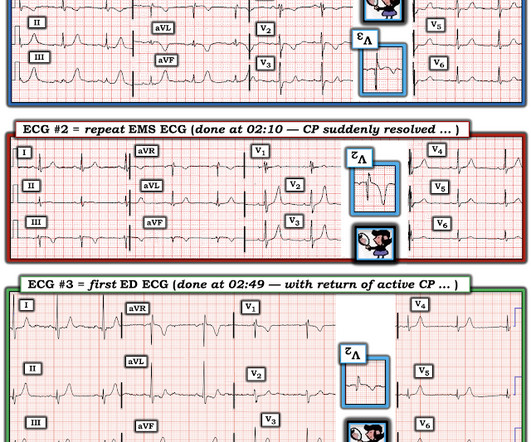
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. Pain was resolving. Diagnosed as Normal by the computer. Troponin negative.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. Learning Points: Serial ECGs can sometimes turn a difficult decision into a very easy one, but not all OMIs will develop into clear STEMIs quickly, and some OMIs never will manifest STEMI at all.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
The lymphocyte-to-C-reactive protein (CRP) ratio (LCR), as a novel inflammatory marker, is associated with the prognosis of patients with ST-segment elevation myocardial infarction (STEMI). This study aims to investigate the correlation between LCR and MVO in STEMI patients undergoing PCI.MethodsThis was a single-center retrospective study.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary disease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
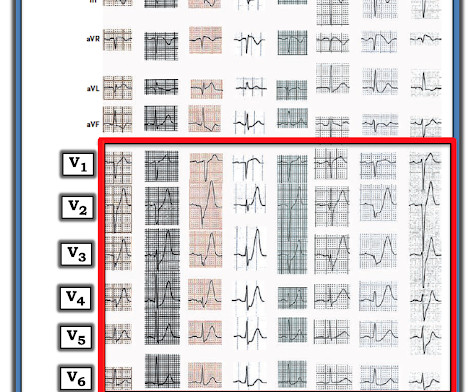
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. He wrote most of it and I (Smith) edited.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardial infarction (STEMI). There were 178 984 patients from 582 US hospitals presenting with STEMI who were included. versus 7.4%,P<0.001), versus 5.1%,P<0.001)
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG. For my clarifying Figure illustrating T-QRS-D ( 2nd bullet ) — See My Comment at the bottom of the page in Dr. Smith’s November 14, 2019 post.
[link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….) it has been subsequently deemed a STEMI-equivalent.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Figure-2: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( See text ). == Addendum Note: Quinidine has a long history of use to treat cardiac arrhythmias and severe malaria. The below ECG was recorded.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? It is often confused with a wide QRS due to conditions such as hyperkalemia. Which artery? There is ST Elevation in every lead except aVR (STD in aVR). Could this be myopericarditis?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Am J Med 2019, 132(5):622-630.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
From My Comment in the November 15, 2023 post in Dr. Smith's ECG Blog: Clinical Points about MINOCA: Given the literature citing a 5-15% estimated incidence of MINOCA in patients initially diagosed as having a STEMI or "NSTEMI" — it is important to be aware of the more common entities associated with this entity ( See Figure-2 ).
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. Really unusual to me that QOH V1 only has low confidence, but at least its correct. During EMS transport, the pain suddenly resolved.
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. For my clarifying Figure illustrating T-QRS-D ( 2nd bullet ) — See My Comment at the bottom of the page in Dr. Smith’s November 14, 2019 post.
His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!) The patient started receiving medications for “STEMI” (including heparin!!!)
This blog post reviews the basics for predicting the " C ulprit" A rtery — as well as the importance of the term, " O MI" ( = O cclusion-based MI ) as an improvement from the outdated STEMI paradigm. For my clarifying Figure illustrating T-QRS-D ( 2nd bullet ) — See My Comment at the bottom of the page in Dr. Smith’s November 14, 2019 post.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content