This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Novartis spun out the testing and development of abelacimab and formed Anthos Therapeutics back in 2019. Novartis initially prioritized its treatments for heart failure and plaque-clogged arteries when it spun-off abelacimab but continued to monitor the Factor XI race, leading to its choice to take the baton back from Anthos.
This registry will aim to provide world-wide physicians the most accurate information on coronary plaque to improve cardiovascular risk prediction and support the selection of patient-specific treatment,” said Dr. De Cecco. The ultimate goal is to positively impact cardiovascular health globally with a reduction in cardiovascular events."
Doctor, do you have any investigation to know how much the total plaque burden is in my coronary artery? I recently read in Forbes Sunday health supplement, It says ,it is better to know the thickness of the cap covering the plaque. to decode the histological, biochemical, pathological secrets within the atherosclerotic plaques.
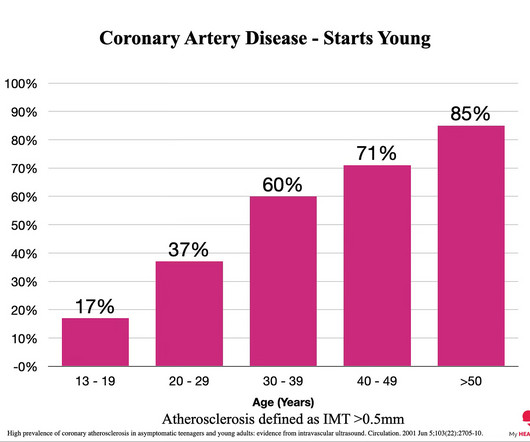
Everyone starts with no plaque in the coronary arteries, but over a long enough time frame, everyone develops plaque in their coronary arteries. By age 80, almost everyone will have evidence of advanced plaque in their coronary arteries, as defined by a cardiac CT 1. Plaque accumulation happens in stages. You got it.
I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment i n the November 14, 2019 post in Dr. Smith's ECG Blog. Non-obstructive coronary disease at the time cardiac cath is done does not necessarily imply there was no plaque rupture with thrombus. A picture is worth 1,000 words.
Lp(a) is emerging as an important, yet under-recognized, potential risk factor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. A focused update to the 2019 NLA scientific statement on use of lipoprotein(a) in clinical practice.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
IVL is a novel approach to lesion preparation of severely calcified plaques in coronary and peripheral vessels. The Henry Ford team performed its first IVL-enabled mitral valvuloplasty back in 2019 and completed its first published case study.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
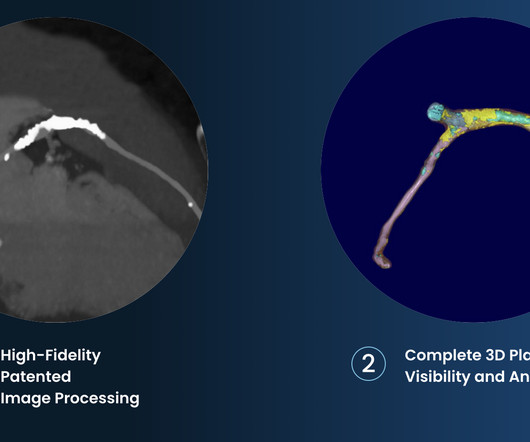
tim.hodson Tue, 10/01/2024 - 10:50 PHOTO CAPTION: The Elucid PlaqueIQ user interface is a fully interactive visualization of the patient’s coronary anatomy, showing specific plaque type and amount across various views to inform physician assessment of risk and patient-specific treatment pathway.
Background Although the impact of hypertension on carotid intima-media thickness (IMT) and plaques has been well established, its association with femoral IMT and plaques has not been extensively examined. Ultrasonography was applied to assess the AS, including thickened IMT (TIMT) and plaque in the carotid and femoral arteries.
FFRCT, coronary plaque, etc). Even with this broader definition, cardiovascular AI’s total share of AI clearances is declining, falling from roughly 25% of clearances in 2018-2019, to 16.5% Cardiovascular AI actually makes up a larger 17.4% in 2020-2022, and 13.5% since the start of 2023.
However, most adults will start to develop advanced plaque in their coronary arteries early in life. By age 66, more than half of all females will have evidence of advanced plaque in their coronary arteries, as seen on a CT calcium score. Coronary atherosclerosis, as evidenced by an abnormal CAC score, is a measure of advanced plaque.
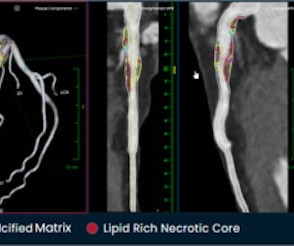
A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. There are 3 types of coronary atherosclerosis visible on CTCA: Calcified Plaque - Easily Identified on both CT CAC & CTCA scans. Subscribe now How Often Does A CT CAC Scan Miss Plaque?
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 Published 2019 Feb 28.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronary artery disease (atherosclerosis/plaque) that might rupture and cause a heart attack. And the less plaque you have, the lower the risk of a heart attack. And it’s also WAY more common.
There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. Figure-1: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( This Table from My Comment in the January 16, 2020 post ).
To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! One of the most common is rupture of a non-obstructive plaque, with thrombus formation and OMI that spontaneously lyses and leaves a wide open artery. It can only be seen by IVUS.
5 High intensity interval training induces beneficial effects on coronary atheromatous plaques – a randomized trial, European Journal of Preventive Cardiology , 2022;, zwac309, 6 FOURIER Steering Committee and Investigators. 2019 Dec 26;381(26):2497-2505. 2006 Apr 5;295(13):1556-65. 2021 May 1;397(10285):1625-1636. N Engl J Med.
While the total body seems to do little in determining cholesterol levels, what is more scientifically shocking is slope of the curve between blood LDL levels and plaque burden is rarely linear. LDL is obviously a target against atherosclerosis. Mind you LDL constitutes.000025% 000025% of total fat.
This is supported by the over 1 million marathon participants worldwide in 2019. Some studies show that high-level endurance runners present with more fibrosis and plaque than age-matched controls (non-runners), data which I’ve covered in detail previously. Is there a downside to this participation?
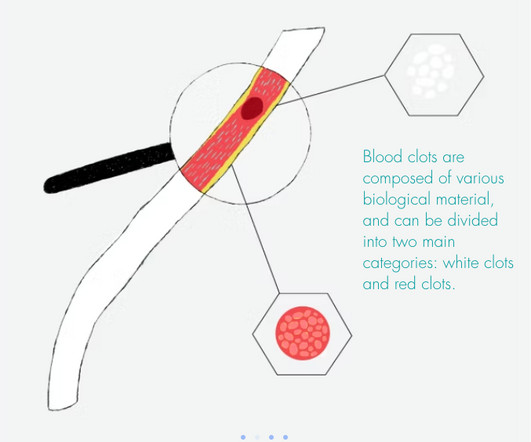
For PAD, the clot-sensing technology is being developed to instantly identify fresh clot and differentiate it from organized clot thrombus poor in RBCs as well as plaque, calcium and other tissue in real-time to inform individualized PAD treatment. Please visit Sensome for more information. Kim, Min Seo et al. Lancet Glob.
Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. JACC 2019 Sep 10;74(10):1290-1300. Angiography Angiography was performed after aspirin and heparin were started.
As an aside, the LCx OMI is a type 2 event, since it is due to supply-demand mismatch from thrombus, and not due to atherosclerotic plaque rupture or erosion). The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity. The January 30, 2018 post — for PTA.
Am J Med 2019, 132(5):622-630. Now there is a paper published in 2019 that proves the point beyond doubt, though makes it clear that this pattern is associated with very high mortality. American Journal of Medicine 132(5):622-630; May 2019. J Electrocardiol 2013;46:240-8 2. Harhash AA, Huang JJ, Reddy S, et al.
Left Circumflex (LCx): Circumflex is a large caliber co-dominant vessel with mild, diffuse plaque There is a single large caliber first obtuse marginal (OM-1) branch that supplies the lateral wall and inferolateral wall via a significant lateral branch, which is occluded in the proximal segment, suggestive of plaque rupture.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Surawicz and Knilans report that intense catecholamine surge, or severe maladjustment of the autonomic nervous system, can manifest “cerebral T waves” in the absence of an acute intracranial process. Furthermore, pertinent electrolyte values (e.g. 40, 1234-41.
But young people do have MI, due to anomalous coronary arteries, coronary artery dissection, Kawasaki dz, even atherosclerotic plaque rupture, and other etiologies. In someone over age 30, MI is far more likely. Under 20, myocarditis is far more likely. You have to be CERTAIN.
Angiogram: Severe coronary artery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronary artery disease. This would be the likely source of the VT. Figure-1: The 2 ECGs in this case ( See text ).
He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. Before transport, a final ECG was recorded: There is, again, inferior reperfusion, but persistent marked anterior STE.
The risk factors for vulnerable carotid plaque were analyzed. Demographic characteristics, vascular risk factors, and the results of preoperative serum biochemistry were measured and collected. A Lasso-logistic regression prediction model was developed and compared with traditional logistic regression models.
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo. Mechanisms of plaque formation and rupture. Coronary plaque disruption.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content