This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( From the information provided — I would not make the diagnosis of acute pericarditis. Figure-1: The initial ECG in today's case.
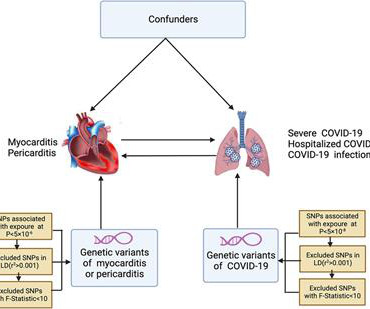
Background & aims Coronavirus disease 2019 (COVID-19) is strongly associated with myocarditis or pericarditis risk in observational studies, however, there are still studies that do not support the above conclusion. 1.12; P = 0.99], pericarditis (OR = 0.90, 95% CI, 0.78–1.04, 1.04, P = 0.17).
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis". ii ) Today's case emphasizes the importance of the history in making the diagnosis of pericarditis.
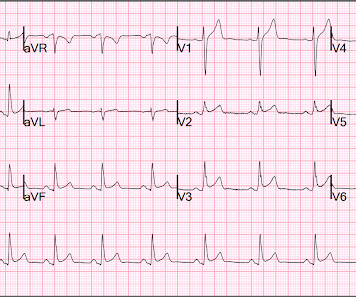
mm has been described in normal subjects) Overall impression: In my opinion and experience, this ECG most likely represents a normal baseline ECG, but with a small chance of pericarditis instead. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant."
The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”. A healthy 45-year-old female presented with chest pain, with normal vitals.
It is easy to say pericarditis in such a case. young male no risk factors and ST-elevation in several leads) As Dr. Smith has emphasized many times you diagnose pericarditis at your patient's and your own peril. Version 1 was not trained to detect myo- or pericarditis. The above ECG was recorded. How did the Queen do?
The undergraduate continues: This new EKG pattern is more suggestive of acute pericarditis. Usually with pericarditis, some degree of PR segment depression is expected. This is typical of pericarditis. But, as I always say, you diagnose pericarditis at your peril. This EKG seems to lack it.
There is a reasonable chance of pericarditis in this case, or this could be a baseline." Sadly, I did not receive enough information to adjudicate whether this patient has pericarditis or not. I sent this to Dr. Smith and this was his response: "Likely pericarditis, but that is perilous. I immediately responded: "cool fake!
Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation. Presence of STD is helpful; absence is not.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present. S mith : there is STE in lead III and reciprocal STD in aVL. This is OMI until proven otherwise.
First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6.
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis. Smith = “You diagnose acute pericarditis at your peril”. We will study this soon with our database.
It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." The clinical presentation is very suggestive of myo-pericarditis. But one should always remember that acute MI is a far more common pathology than myo- or pericarditis. Pericarditis?
She was diagnosed with pericarditis and spent one day in the hospital without events. Much more classic findings of pericarditis. Learning Points: Pericardial effusion is a key piece of information for the diagnosis and prognosis of pericarditis. Another ECG was performed, and this time was noted to be markedly abnormal.
Echo does not necessarily differentiate acute MI from pericarditis: both may have wall motion abnormalities. This is why I frequently write: "You diagnose pericarditis at your peril." I have therefore found this sign of limited usefulness in most instances when contemplating a diagnosis of acute pericarditis or myocarditis.
Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? But it is very distinct from hyperkalemia (and anything else, including VT), and such confusion can only be due to lack of familiarity, because, if you look closely, its morpholgoy is very different from anything else. So this is STEMI, right? Which artery?
Traditionally used as an anti-inflammatory for pericarditis (inflammation of the lining of the heart), it has recently been shown to result in fewer major heart events in those with a recent heart attack. 2019 Dec 26;381(26):2497-2505. It is an easy win, frequently missed. 2021 May 1;397(10285):1625-1636. N Engl J Med.
Fortunately, there was an ECG from about a year prior: And here is one from about 10 years prior: You can see here that the computer says "suggests pericarditis" but that I changed it to early repolarization. Just because there is diffuse ST elevation does NOT mean it is pericarditis.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. 2019 Apr;21(5):253-258. Look at the STE in lead II, aVF. Anatol J Cardiol.
The "flu-like" illness suggests myo- or pericarditis, but that would be a diagnosis of exclusion. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity. The September 22, 2019 post — intermittent ST-T wave artifact. The case continues.
Pericarditis? A straight ST segment virtually never happens in inferior ST elevation that is NOT due to OMI (normal variant, pericarditis) 4. 60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. Time zero What do you think? There is inferior ST elevation. Is it normal variant?
Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chest pain. Initial troponin came back negative." Sodium channel blockade effect from unidentified drug?" "In
There is also mild pericardial enhancement consistent with pericarditis. He later underwent an MRI: 1) Mildly decreased LV function with no focal wall motion abnormalities 2) Patchy intramyocardial delayed enhancement compatible with myocarditis. Overall findings are consistent with myopericarditis.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. ST depression. Myocardial Contusion?
This is the most important exception to the classic teaching of "diffuse STE without reciprocal depression is less likely ACS, more likely pericarditis".
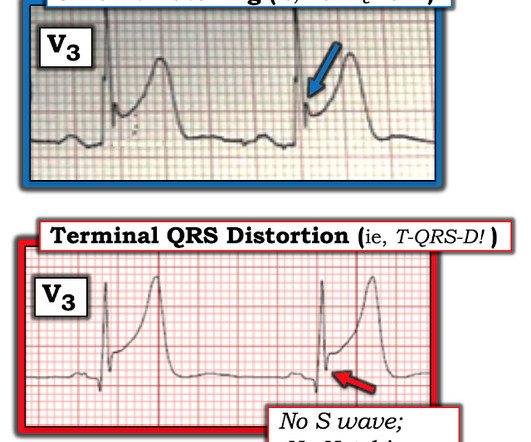
You do NOT see this in normal variant STE, nor in pericarditis. Here is the computer interpretation: (Veritas algorithm) This is what I said: "This is diagnostic of an acute inferior MI. There is upsloping ST elevation in III, with reciprocal ST depression in aVL.
Though less prevalent in younger patients, occlusion MI may occur and requires the same early interventions as older patients. - - Pericarditis and myocarditis should be a diagnosis of exclusion. I've listed potential causes of acute pericarditis in My Comment at the bottom of the page in the June 11, 2022 post in Dr. Smith's ECG Blog.
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But STEMI criteria ignore all this and look at ST segments in isolation. Based on STEMI criteria and unhelpful computer interpretation, the patient was rushed to the cath lab.
Despite apparently hearing the above history together with two diagnostic ECGs and a troponin compatible with OMI, the cardiologist thought the ECG represented pericarditis and recommended echocardiogram. The emergency physician consulted cardiology. Several hours passed with no documentation as to the reason for delay.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content