This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
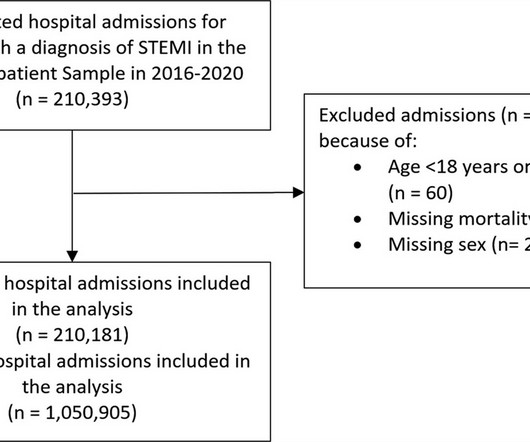
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2%
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
This was a machine read STEMI positive OMI. the investigators reviewed outcomes in 118 patients presenting with NSTEMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below.
1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. References: 1. Available from: [link] [link] 2.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Am J Med 2019, 132(5):622-630.
“ Since Intravenous lysis looks too simplistic, that do not need expertise, and lacks a commercial trail, it is wrongly depicted as inferior management strategy in STEMI “ Every one of us is equally responsible for this sorry state of affairs. In LAD STEMI time is more crucial. Circulation 2006;114:2019-25
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. First trop was 90 ng/L (normal <16 in females) and peak was 7,400 ng/L.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. Outcome of our case Once the type 2 SCAD was identified, the heparin drip was stopped. JACC 2019 Sep 10;74(10):1290-1300. Lobo et al. where more than 3/4 of cases were NSTEMI).
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Other outcome information is not available. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. No prior ECG was available.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. References: 1. Available from: [link] [link] 2.
It is difficult to describe exactly why, but is something that simply comes with time, after following up hundreds of cases to see the ECG progression and patient/angiographic outcomes. This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. Angiogram is normal.
Emergent cardiac outcomes in patients with normal electrocardiograms in the emergency department. We wrote this Editorial in the Journal of Electrocardiology in 2019. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI.
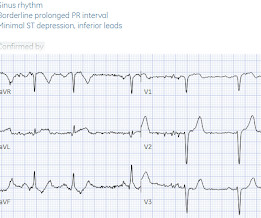
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
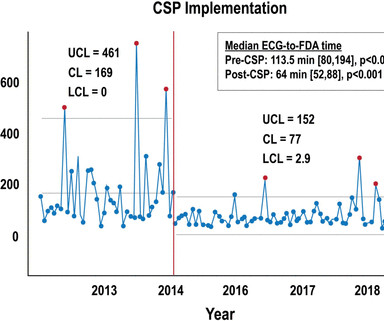
Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre. Key metrics and clinical outcomes were compared before and after CSP implementation.
Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients. All patients with STEMI underwent CPFD-caIMR and MVO assessment.
A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab.
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary disease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
Introduction Despite ongoing efforts to minimize sex bias in diagnosis and treatment of acute coronary syndrome (ACS), data still shows outcomes differences between sexes including higher risk of all-cause mortality rate among females. The primary outcome was in-hospital mortality.
However, in multiple studies, even in the absence of AMI, both acute and chronic myocardial injury (as diagnosed by any elevated cTn) are powerful markers of adverse outcomes in both the short and long term. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 3–8 Shi et al. Guo T, Fan Y, Chen M, et al.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI. Angiogram: LM 30% ostial.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. But it does show a strong association of better outcome with lidocaine vs. amiodarone. Return of spontaneous circulation (ROSC) was the primary outcome. Smida T et al.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference. HyperKalemia with Cardiac Arrest. References 1.
It is a long read, meant only for those who want to know the hidden intricacies in the concept of “Time window” in STEMI and its important Implication in patient care. [08/11, Stronger predictor of outcomes (mortality, myocardial damage). 2019 ESC) emphasize FMCTB and STB times. Symptom-to-Balloon (STB) time 1.
Was her outcome to be expected for ostial RCA OMI? Whereas the patient's initial ECG shows sinus rhythm and nonspecific ST-T wave abnormalities just 24 minutes later , there is now profound bradycardia with a junctional escape rhythm ( YELLOW arrows highlighting retrograde P waves ) and obvious findings of an acute inferior STEMI.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content