This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundCurrent research suggests that microvascular obstruction (MVO) following the first percutaneous coronary intervention (PCI) in myocardialinfarction patients is closely related to inflammatory responses. The predictive model incorporating LCR enhances the ability to predict MVO occurrence in patients with STEMI post-PCI.
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardialinfarction (STEMI) and multivessel coronary disease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
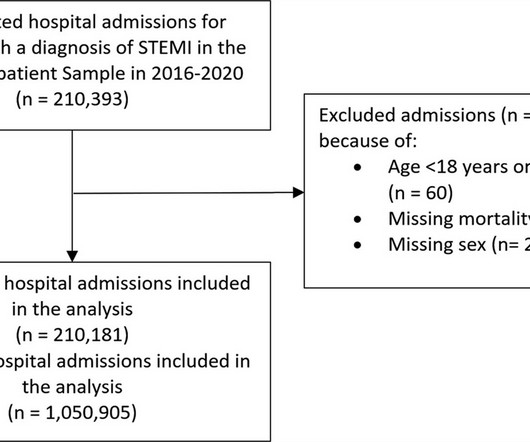
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardialinfarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% for patients admitted in 2016–2019 period. vs. 10.7%; P < 0.001).
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
BackgroundThere may be variability in willingness to perform percutaneous coronary intervention (PCI) in higherrisk patients who present with STsegmentelevation myocardialinfarction (STEMI). There were 178 984 patients from 582 US hospitals presenting with STEMI who were included. versus 7.4%,P<0.001),
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
Patients with ST-segment–elevation myocardialinfarction undergoing primary percutaneous coronary intervention were randomly assigned by center to receive low-dose PPA or matching placebo for at least 48 hours. mg·kg·h of bivalirudin intravenously). mg·kg·h of bivalirudin intravenously). to 1.57]).
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardialinfarction" but do not discuss it as a "STEMI equivalent."
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
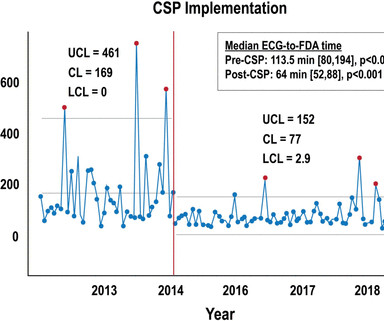
Background Patients who experience in-hospital ST-segment elevation myocardialinfarction (iSTEMI) represent a uniquely high-risk cohort owing to delays in diagnosis, prolonged time to reperfusion and increased mortality. Quality initiatives aimed at improving the care of this vulnerable, yet understudied population are needed.
associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. MINOCA I do not have the bandwidth here to write a review of MINOCA.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
“ Since Intravenous lysis looks too simplistic, that do not need expertise, and lacks a commercial trail, it is wrongly depicted as inferior management strategy in STEMI “ Every one of us is equally responsible for this sorry state of affairs. In LAD STEMI time is more crucial. Circulation 2006;114:2019-25
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Barely any STE, and thus not meeting STEMI criteria. Read our recent editorial: Hyperacute T-waves Can Be a Useful Sign of Occlusion MyocardialInfarction if Appropriately Defined. Read our recent editorial: Hyperacute T-waves Can Be a Useful Sign of Occlusion MyocardialInfarction if Appropriately Defined.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). The below ECG was recorded. Inotropic medication was continued.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The EMS crews were correct moving forward with STEMI activation. 1] Driver, B.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Am J Med 2019, 132(5):622-630.
The ECG is diagnostic of occlusion myocardialinfarction (OMI). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The overall read is OMI with HIGH confidence. == Below is the ECG of Patient #2 — as interpreted by the QOH.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
If it is STEMI, it would have to be RBBB with STEMI. Only 5-18% of ED patients with chest pain have a myocardialinfarction of any kind. The patient presented with chest pain. Here is the ECG: What do you think? I frankly did not know what to think. Is it Brugada pattern? But in a very unusual pattern. Only 1-5% have OMI.
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. It can only be seen by IVUS.
See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. And there is ST depression in V2 and V3, all but diagnostic of posterior OMI.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. JAMA Intern Med 2019 9. Lancet 2015 6. Patel J, Alattar F, Koneru J, et al.
The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here. Considerations on the naming of myocardialinfarctions. 2019 Apr;21(5):253-258. He arrived to our hospital one hour later. J Electrocardiol. 2022 Mar-Apr;71:44-46. doi: 10.1016/j.jelectrocard.2022.01.006.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chest pain from an 8/10 to 4/10. NTG drip started. Pain better still. Is this OMI?
A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. Revascularization in Patients With Spontaneous Coronary Artery Dissection and ST-Segment Elevation MyocardialInfarction. JACC 2019 Sep 10;74(10):1290-1300. A study by Hassan et al.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
We wrote this Editorial in the Journal of Electrocardiology in 2019. Available from: [link] Excerpt: "To illustrate the limitations imposed by sample size, recent data from our institution reveal that we identify approximately 225 type I myocardialinfarctions (MI) in a typical year. Litell JM, Meyers HP, Smith SW.
I describe and illustrate in detail my approach to incorporating these criteria in My Comment at the bottom of the December 16, 2019 post in Dr. Smiths ECG Blog. However, the cath lab activation was cancelled by the on-call interventionalist who felt the diagnosis of acute STEMI could not be made because of the LBBB.
V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific. Posterior infarctions often ( though not always ) result in an increase in R wave amplitude in anterior leads.
The important point for our purposes is that they do no represent myocardialinfarction. International Journal of Cardiology 2019. Anterior STEMI? Dr. Smith note: I wouldn't necessarily consider this ENTIRELY "benign." It may even be that patients with ECGs with this morphology have a higher long term risk. Paana et al.
Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk. Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y. Murakami M. Acute Cardiovascular Care 2014;3(4):317-325.
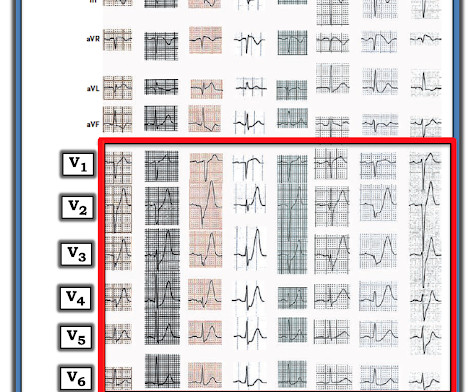
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
STEMI negative : the EMS automated interpretation read, “STEMI negative. Inferior infarct, age undetermined. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardialinfarction presented to the ED with chest pain at 2343. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent").
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Acute myocardialinfarction triggered by emotional stress.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. The September 22, 2019 post — intermittent ST-T wave artifact.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content