This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Even with tachycardia and a paced QRS duration of ~0.16 J Am Coll Cardiol. 1 for a rate ~75/min 1.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Are you confident there is no ischemia? Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Is this: 1.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Additionally, the qR morphology, particularly in a patient with right bundle branch block (RBBB) type wide QRS complex tachycardia (WQCT), lends further support for VT. What is the rhythm?
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
A 50-something male with unspecified history of cardiomyopathy presented in diabetic ketoacidosis (without significant hyperkalemia) with a wide complex tachycardia and hypotension. Analysis: there is a wide complex tachycardia. This was the interpretation I put into the system: WIDE COMPLEX TACHYCARDIA. It is regular.
With normal EF the tachycardia is not compensatory. The same reciprocal relationship is seen in severe subendocardial ischemia, just with opposite vector direction where V1 can show ST elevation) Below you can find the 3D model of the heart and coronary vessels. And the patient has sinus tachycardia. ( HR about 90-100/min.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Am J Med 2019, 132(5):622-630.
Here was the ECG: There is sinus tachycardia. Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. This was sent by a reader. A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. and K was normal. This is "Shark Fin" morphology.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Tachycardia and ST Elevation. She was discharged home. Christmas Eve Special Gift!!
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
See this case, where a patient with BTWI morphology and dramatic EKG changes within minutes is diagnosed with myocarditis: [link] com/2019/07/what-does-this- ecg-with-significant-st.html EKG 3 also has a saddleback morphology in V2, which is only rarely due to OMI. Still, such dramatic changes cannot be overlooked. It was stented.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. Hypokalemia c.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
No more abnormal U-waves == MY Comment, by K EN G RAUER, MD ( 11/18/2019 ): == LOTS of great points regarding use of the ECG in association with electrolyte abnormalities. This is often quite challenging to recognize — but the finding of negative U waves in a patient with chest pain is highly suggestive of ischemia ! second ).
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. In lead III there is the tiniest possible amount of STE which is difficult to measure due to the very low-voltage.
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiac arrest — and especially Hyperkalemia. Sinus Tachycardia ( common in any trauma patient. ).
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
ECG is consistent with severe hypokalemia and/or hypomagnesemia causing prolonged QT (QU) at high risk of Torsades (which is polymorphic ventricular tachycardia in the setting of a long QT interval). Polymorphic Ventricular Tachycardia Long QT Syndrome with Continuously Recurrent Polymorphic VT: Management Cardiac Arrest.
There is a run of polymorphic ventricular tachycardia — which given the QT prolongation, qualifies as Torsades de Points ( TdP ). This patient was having recurrent episodes of polymorphic ventricular tachycardia with an underlying long QT interval ( = Torsades des Pointes ). ECG #2 Interpretation of ECG #2: Underlying sinus rhythm.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is no evidence of infarction or ischemia. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. There are nonspecific ST-T abnormalities. This seems to me to be very unlikely.
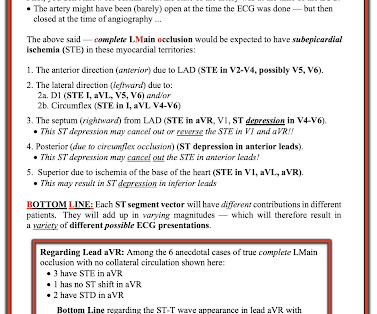
The terminology favored to describe these ECG findings is diffuse subendocardial ischemia ( See ECG Blog #271 — for more on diffuse subendocardial ischemia ). Figure-3: Reasons for the varied ECG presentation of acute LMain occlusion — with this summary synthesized from Dr. Smith’s 8/9/2019 post in his ECG Blog.
Cardiovascular Implications of Fatal Outcomes of Patients With Coronavirus Disease 2019 (COVID-19). Association of Coronavirus Disease 2019 (COVID-19) With Myocardial Injury and Mortality. Cardiac troponin I in patients with coronavirus disease 2019 (COVID-19): Evidence from a meta-analysis. Guo T, Fan Y, Chen M, et al.
This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2] 2] But there is also Sinus Tachycardia! Chapter 6: Introduction to Myocardial Ischemia and Infarction.
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. This is a perfect indication for atropine.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. A rectal temperature was obtained which read 107.9
It doesn’t require any extraordinary intelligence to conclude any chronic focal atrial tachycardia can get degenerated to AF in the long run. In that case, the famous atrial tachycardia localizing map from Peter Kistler et al from Australia JACC 2006 holds good for location AF focus too. 2019 Nov, 5 (11) 13281330 2.
It is a wide complex regular tachycardia at a rate of 120. Is it ventricular tachycardia? I fear that many learners would also not easily recognize where the QRS actually ends, and I fear that some may think that this is ventricular tachycardia due to inability to distinguish QRS from ST segment. The ST Elevation is NOT typical.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Here is the final angiogram following placement of a stent in the ostial RCA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content