This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
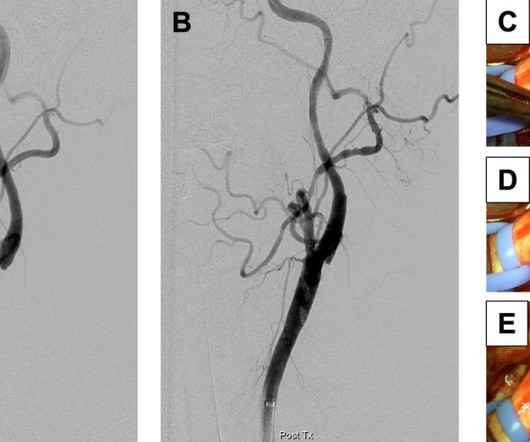
To our knowledge, no studies have directly compared the right and left TRA for carotid artery stenting (CAS). The right TRA was performed as a first-line approach from 2019 to 2021, with the left TRA being used thereafter. All carotid stenoses were successfully dilated.
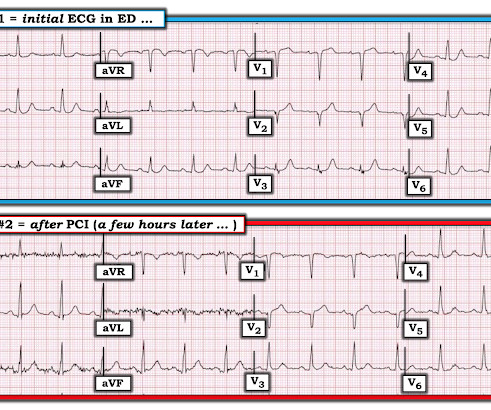
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? The last echocardiography 12 months ago showed HFmrEF.
5 ICSS‐ MRI study (International Carotid Stenting Study Magnetic Resonance Imaging Study), indicated that patients with periprocedural hemodynamic depression had decreased cerebral blood flow and increased the risk of new lesions in imaging.6 This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. 2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. But it is still STEMI negative.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Whether these EKGs show myocarditis, a normal variant, or something else, they are overall not typical of transmural ischemia of the anterior or high lateral walls. It was stented.
One stent was deployed with restorative TIMI-0 flow. Accurate identification is absolutely necessary as this pattern can be easily misinterpreted for something less nefarious: for example, generic “subendocardial ischemia.” However, when the Troponin I returned 8.4 The red arrow shows a 90% LAD occlusion at the D1 branch.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. A mid-LAD culprit lesion was identified and stented. References Naidu, S. Tower-Rader, A.
Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. This patient's ischemia was so brief that it did not cause any myocardial stunning. This patient's ischemia was so brief that it did not cause any myocardial stunning.
60-something with h/o MI and stents presented with chest pain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. More likely, these T waves probably reflect ischemia of uncertain age. Time zero What do you think? There is inferior ST elevation. Pericarditis?
This transmural ischemia, but not necessarily completed infarction (yet). See more images of this case at Gopal's Spectral CT Blog: It's all about confidence With continued symptoms, an elevated troponin, and no other explanation, this is acute MI with ongoing ischemia until proven otherwise.
It could at least say: "ST Elevation, consistent with normal variant," or "consistent with ischemia or normal variant," or "consistent with early repolarization." Some normal STE is not due to ischemia at all. 100% proximal LAD successfully stented. But it simply says "normal." Some patient's baseline ECG has zero STE.
They found 100% acute mid-LAD Occlusion MI, stented with excellent angiographic result. Ongoing ischemia (by symptoms, ECG, or troponin) despite maximal medical management is an indication for emergent cath lab activation. == MY Comment by K EN G RAUER, MD ( 8/15/2019 ): == Once again, the w rong q uestion was a sked in this case.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. The culprit lesion was opened and stented. For more on this mirror-image opposite ST-T wave relation in leads III vs aVL — See My Comment in the March 8, 2019 and August 9, 2018 posts in Dr. Smith's ECG Blog ).
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. 5 ISCHEMIA Research Group.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
100% proximal LAD thrombotic occlusion with TIMI 0 flow was found and stented with excellent angiographic result and TIMI 3 flow. When in doubt, record serial ECGs and watch out for signs of ischemia despite medical management. == Comment by K EN G RAUER, MD ( 7/11/2019 ): == Our thanks to Drs. Cath images: Before intervention.
Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. It was opened and stented. link] == MY Comment, by K EN G RAUER, MD ( 12/17/2019 ): == Great case about some subtleties in association with LBBB.
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. He was successfully stented. Smith pointed out that while atropine may may result in slightly more oxygen demand, the increase in cardiac output and in blood pressure would increase overall coronary perfusion and decrease ischemia.
distal stent patent. Given our concern about possible subtle high-lateral OMI — this raises the question whether the upright T waves in leads V1 and V2 of this 1st ECG might be abnormal and reflect ischemia. Repeat ECG shows modest ST elevation in I and aVL and depression in inferior leads." The cath lab was activated.
His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria. There is evidence of transmural ischemia of the posterior wall as well. Leads V1 to V4 have down-up shaped T waves typical of ischemia and atypical of LBBB.
It is not clear by her note what she meant by this (whether or not she recognized this EKG as diagnostic of transmural ischemia, and if so, of what territory) but emergent reperfusion therapy was not pursued. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. Subendocardial ischemia does not localize.
Pasarikovski, Neurology: Clinical Practice 2019 How does it appear in carotid angiogram and in real time per-operative ? Management The web can create a flow disturbance, potentiating local thrombus formation, which can embolize producing resulting in cerebral ischemia. Christopher R. Reference 1.Rainer Rainer W.G., Cramer G.G.,
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). That the chief complaint of today's patient was acute CP ( C hest P ain ) with a history of known coronary disease and LAD stent placement a few weeks earlier. He appeared critically ill.
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The August 26, 2019 post — baseline artifact.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content