This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Cardiovascular disease is the most common cause of death and disability globally, largely driven by myocardialinfarction and ischemic stroke caused by atherosclerosis (plaque build-up in the arteries). 6 (3) (2019). 2017 23, April 2020; Available from: [link]. Cardiovasc.
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. The ECG is diagnostic of occlusion myocardialinfarction (OMI).
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. What do you think?
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardialischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024. month follow-up.
Troponin T peaked at 38,398 ng/L ( = a very large myocardialinfarction, but not massive-- thanks to the pre-PCI spontaneous reperfusion, and rapid internvention!! ). There is no definite evidence of acute ischemia. (ie, Some residual ischemia in the infarct border might still be present.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely. NTG drip started.
This suggests further severe ischemia. associated typical MyocardialInfarction therapies such as statins and ACE inhibitors with significantly decreased 1 year mortality in MINOCA patients, which suggests that they do indeed have a similar pathophysiology to MI patients with obstructive coronary disease. Downstream vasospasm?
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 2019 Sep 10;140(11):e649-e650] [published correction appears in Circulation. Published 2019 Feb 28. 4 In the U.S. 12 Colchicine, 0.5
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Am J Med 2019, 132(5):622-630.
When “spot diagnosing” precordial ST-depression I instinctively evaluate aVR for any corresponding ST-elevation to see if an emerging pattern of broad subendocardial ischemia can be appreciated, in which the ST-depression should be otherwise global and demonstrably maximal in Leads II and V5. ST-elevation, etc.) is present. 1] Driver, B.
or basilar ischemia. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. Rather than loss of both a J wave and S wave — there is a "slur" ( J-point equivalent ) in lead V2 of ECG #2 ( See My Comment in the November 14, 2019 post for illustration of T-QRS-D ).
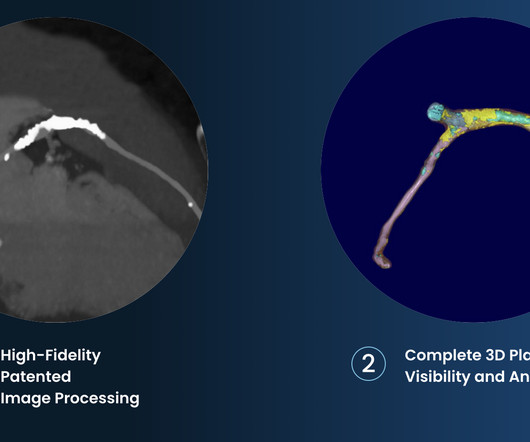
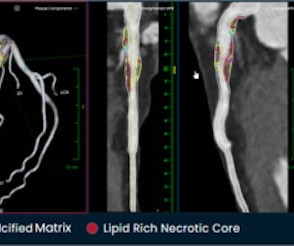
The company is also pursuing an indication for non-invasive measurement of fractional flow reserve (FFR CT ), uniquely derived from its PlaqueIQ technology, to measure coronary blockages and the extent of ischemia. 6 (3) (2019). Hafiane, Vulnerable plaque, characteristics, detection, and potential therapies , J. Cardiovasc.
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. I believe this is by far the most common outcome for this patient around the world in 2019. So what will you do for this patient?
ST-elevation myocardialinfarction after pharmacologic persantine stress test in a patient with Wellens’ syndrome. JAMA Intern Med 2019 9. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction. Was this objective evidence of inducible ischemia accompanied by chest pain?
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. SCAI 2019 Catheter Cardiovasc Interv.2019;94:29–37 PMID: 35743628; PMCID: PMC9224589. Circ Cardiovasc Qual Outcomes.
LAD 80% mid LCx occluded mid (acute infarct lesion) RCA 80% mid. PCI mid LCx So this is an OMI (Occlusion MyocardialInfarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk.
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. It helps a little bit.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in Emergency Department COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. In normal times, the most common use of cTni is in diagnosing, or ruling out, acute myocardialinfarction (AMI, a subcategory of acute myocardial injury.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. JACC 2019 Sep 10;74(10):1290-1300. There is also a Q-wave in III. There is also subtle STD in V3-V5.
Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs.
There is no ST depression in V6, II, III, or aVF, and no significant ST elevation in aVR, all confirming that the ST vector is not consistent with diffuse subendocardial ischemia, but rather a focal ST vector pointed at the posterior wall. There is sinus rhythm with normal QRS complex and ST depression in V2-V5, maximal in V3-V4.
Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With MyocardialInfarction With Nonobstructive Coronary Artery Disease. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! Lindahl et al.
2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. 5 ISCHEMIA Research Group. 5 ISCHEMIA Research Group. Medicine (Baltimore). 2022 Sep 16;101(37):e30583. N Engl J Med. 2018 Sep 6;379(10):924-933. Eur Heart J.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
Appearance of Abnormal Q Waves Early in the Course of Acute MyocardialInfarction: Implications for Efficacy of Thrombolytic Therapy.” Pain will resolve with completed infarct or with resolution of ischemia. This looks like infarct completion. ECG recorded at 7 hours All active ischemia is gone. Maynard, G.
Chest pain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated. Comparison of the QRS Complex, ST-Segment, and T-Wave Among Patients with Left Bundle Branch Block with and without Acute MyocardialInfarction.
RCA ischemia often results in sinus bradycardia from vagal reflex or ischemia of the sinus node. Smith pointed out that while atropine may may result in slightly more oxygen demand, the increase in cardiac output and in blood pressure would increase overall coronary perfusion and decrease ischemia.
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardialinfarction presented to the ED with chest pain at 2343. His triage EKG is shown below: There is left bundle branch block, so the EKG must be evaluated for ischemia by Smith-modified Sgarbossa criteria.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. SanzRuiz, R., Solis, J., &
Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The September 22, 2019 post — intermittent ST-T wave artifact.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content