This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BACKGROUND:Lower-limb amputation rates in patients with chronic limb-threatening ischemia vary across the United States, with marked disparities in amputation rates by gender, race, and income status. Circulation: Cardiovascular Interventions, Ahead of Print. Mean age, 76.6
It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome. Smith, this can be accomplished by either using beta-one agonists or temporary transvenous pacing. J Am Coll Cardiol.
TIB in the intervention group was significantly reduced at the 1,2, and 4-week marks post-intervention and exhibited a higher effective rate of total myocardial ischemia load reduction. The control group underwent a standard rehabilitation program, while the intervention group participated in an individualized exercise rehabilitation program.
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
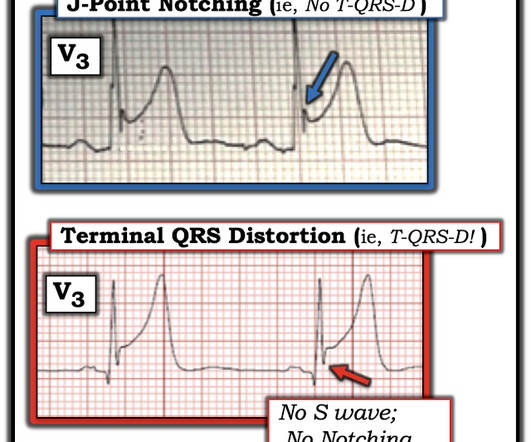
For my clarifying Figure illustrating T-QRS-D ( 2nd bullet ) — See My Comment at the bottom of the page in Dr. Smith’s November 14, 2019 post. = ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
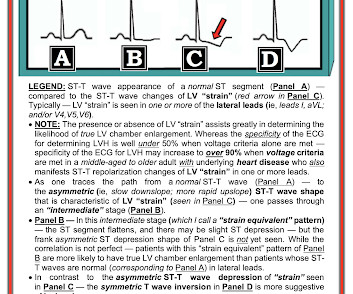
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. Please see ECG Blog #73 for additional details ).
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. As suggested by Figure-4 below in the ADDENDUM — assessment of the ST-T waves in leads V2,V3 and V5,V6 — is consistent with ischemia and / or LV "strain".
In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. We've highlighted a considerable number of acute RV MI cases in Dr. Smith's ECG Blog ( See the October 7, 2019 and May 10, 2024 posts , to name just two ).
In any case, the ECG is diagnostic of severe ischemia and probably OMI. So this could be myocarditis but in my opinion needs an angiogram before making that diagnosis. == Dr. Nossen Comment/Interpretation: Evaluation of ischemia on an ECG can be very challenging. Concordant STE of 1 mm in just one lead or 2a.
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy? How can you better assess the ST segments?
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Subendocardial ischemia results in ST depression, but unfortunately, and rather mysteriously, it does not localize to the ischemic wall. Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
We sought to evaluate PFO closure rates and indications relative to the timing of regulatory approval and publication of key randomized trials.Methods:We performed a retrospective cohort study using the OptumLabs Data Warehouse of US commercial insurance enrollees from 2006 to 2019. per 100 000 person-years in 2019. female, 29.2%≥60
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Am J Med 2019, 132(5):622-630.
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
The same reciprocal relationship is seen in severe subendocardial ischemia, just with opposite vector direction where V1 can show ST elevation) Below you can find the 3D model of the heart and coronary vessels. Each main coronary artery (LAD, RCA and LCx) are shown in separate images.
IntroductionTransient Ischemic Attack (TIA) is a common neurologic condition characterized by temporary, focal cerebral ischemia that results in reversible neurological deficits without tissue infarction. from 2016‐2019 and secondary diagnosis of T2DM. Diabetics were more likely to be younger (70.43
Learning Point: Concordant ST segment elevation can arise from profound ischemia triggered by ventricular tachycardia (VT), or it may represent an exaggerated basal ST change accompanying tachycardia. The patient rapidly regained consciousness, reporting no residual pain. A peak troponin level of 70 ng/L was observed.
This study aimed to evaluate the safety and technical feasibility of left TRA-CAS in comparison to right TRA-CAS.Methods:We conducted a retrospective review of consecutive patients who underwent TRA-CAS using a 6-French Simmons guiding sheath between 2019 and 2024. Patients who underwent proximal balloon-protected CAS were excluded.
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. She was taken to the cath lab and her coronaries were clean!! There was no MRI, but the presumptive diagnosis is myocarditis. I have seen this pattern in severe acute AI also."
This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7 7 Clinical indicators like delirium can play a role in evaluating for delayed cerebral ischemia and infarction leading to timely management of vasospasms.5,8,9
or basilar ischemia. Rather than loss of both a J wave and S wave — there is a "slur" ( J-point equivalent ) in lead V2 of ECG #2 ( See My Comment in the November 14, 2019 post for illustration of T-QRS-D ). EKG on arrival to the ED is shown below: What do you think? However, T waves do not appear to be hyperacute or hyperkalemic.
2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. The absence of STE in V7-V9 is often due to resolution of ischemia, as seen by resolution of ST depression in V7-V9. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al.
Stroke: Vascular and Interventional Neurology, Ahead of Print. Descriptive statistics including medians (interquartile range) and proportions were used as appropriate.
That said — I did not interpret these differences as the result of acute ischemia. An additional criterion that has sometimes been cited as helpful for making the diagnosis of acute Pericarditis — is the ST/T Wave Ratio in Lead V6 ( Please see My Comment at the BOTTOM of the page in the December 13, 2019 post of Dr. Smith's ECG Blog ).
Background:Myocardial infarction with nonobstructive coronary artery disease (MINOCA) is a special syndrome with clear evidence of myocardial ischemia, but no clear stenosis of coronary artery imaging sign. Circulation, Volume 150, Issue Suppl_1 , Page A4143007-A4143007, November 12, 2024. month follow-up.
Final diagnosis of cerebral ischemia was made in 662/1043 patients (63.5%) and stroke mimic was diagnosed in 381/1043 patients (36.5%). Detailed chart review was conducted to extract both the variables needed to apply the mimic scales the final diagnosis confirmed by final imaging and discharge diagnosis (cerebral ischemic vs stroke mimic).
BACKGROUND:Abnormal orthostatic blood pressure (BP) regulation may result in cerebral hypoperfusion and brain ischemia and contribute to dementia. The primary outcome was adjudicated dementia ascertained through 2019.RESULTS:Among Hypertension, Ahead of Print. RESULTS:Among 11 644 participants (mean [SD] age, 54.5 [5.7]
A majority (62.5%) of those presenting with ‘normal’ ECGs had the cath lab activated without any ECG being labeled ‘STEMI’ by automated interpretation – based on signs of Occlusion MI including ECG changes, regional wall motion abnormality on bedside ultrasound, or refractory ischemia. 2019 ; 54 : 79 - 81. Acad Emerg Med.
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ). My approach (which is not unique) is rate, rhythm, axis, hypertrophy, intervals. (In
Though this association may be related to impaired cerebral oxygen delivery, it is unclear whether these changes relate to cerebral ischemia. Patients who had a brain MRI and serial hemoglobin measurements were included.
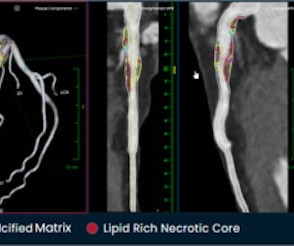
The company is also pursuing an indication for non-invasive measurement of fractional flow reserve (FFR CT ), uniquely derived from its PlaqueIQ technology, to measure coronary blockages and the extent of ischemia. 6 (3) (2019). Hafiane, Vulnerable plaque, characteristics, detection, and potential therapies , J. Cardiovasc.
So this relatively long QT interval is NOT due to ischemia but may be a result of CO Toxicity. Read more about CO poisoning and cardiac ischemia here (ECG is pasted below): What is the treatment for this subendocardial ischemia? Yelken B et al. Routine ECG recorded before hyperbaric therapy.Are they related?
JAMA Intern Med 2019 9. We are told that the Stress Echo that was performed showed objective evidence of inducible ischemia ( confirmed apparently by both wall motion abnormalities and ECG changes ). Was this objective evidence of inducible ischemia accompanied by chest pain? Gulati M, Levy P, Mukherjee D, et al.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
This can be simply a equivalent of HT, with no true supply side ischemia with LVF with global ST depression ) Management *More or less similar to STEMI with aggressive opening of culprit lesions with few differences. SCAI 2019 Catheter Cardiovasc Interv.2019;94:29–37 PMID: 35743628; PMCID: PMC9224589. Circ Cardiovasc Qual Outcomes.
This suggests further severe ischemia. There is 1 mm of ST segment elevation in lead aVR — which in the context of ST segment flattening in most other leads, suggests that there may be a component of subendocardial ischemia from underlying coronary disease. Detailed coronary artery evaluation not performed. Downstream vasospasm?
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. Hypokalemia c.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content