This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
EKG with paced complexes shown below shows much narrower QRS complex and echocardiogram showed improved LV systolic function primarily due to improvement in LV dyssynchrony. (J Applying my method to the March 19, 2019 case that I show in Figure-1 the rhythm in this Figure-1 ECG is regular, with an R-R interval just under 4 large boxes.
What do you think the echocardiogram shows? In the March 9, 2020 post of Dr. Smith’s ECG Blog — Dr. Smith presented results from a 2019 article by Harhash et al, that confirm how the ECG pattern shown in Figure-1 does not represent acute LMain occlusion — but rather the differential diagnosis that I show above. NTG drip started.
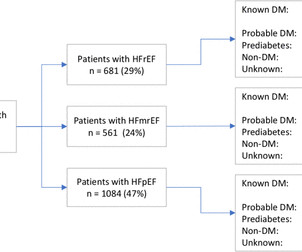
Patients’ HF phenotype was determined using the latest available echocardiogram. Results In total, 2326 patients (59% male, mean age 76±13 years) with HF and at least one echocardiogram were assessed. The number of patients with previous DM diagnosis was assessed.
Methods Retrospective chart review of 200 patients admitted for ADHF from 2018 to 2019 with transthoracic echocardiogram during index hospitalisation. The aim of this study was to assess the relationship between IVC diameter, clinical variables and ADHF rehospitalisations. Charts were assessed for ADHF rehospitalisation within 1 year.
The March 31, 2019 post in Dr. Smith's ECG Blog — My Comment ( at the bottom of the page ) illustrates the potentially misleading effect the pre-hospital ECG may have in patients with LVH , by cutting off S wave voltage in the anterior leads. Cardiac cath showed normal coronary arteries.
The aim was to assess the burden and clinical correlates of VHD in a highly diverse area of the United States.Methods and ResultsIndividuals with echocardiographic diagnosis of native VHD between January 2010 and December 2019 at a quaternary care health system of the Bronx (New York, USA) were included.
His echocardiogram showed normal wall motion. From My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog: A subject well worth periodic review — is the concept of Terminal QRS Distortion ( T-QRS-D ). Figure-4: I've labeled the first 2 ECGs shown in the November 14, 2019 post ( See text ).
See this case, where a patient with BTWI morphology and dramatic EKG changes within minutes is diagnosed with myocarditis: [link] com/2019/07/what-does-this- ecg-with-significant-st.html EKG 3 also has a saddleback morphology in V2, which is only rarely due to OMI. Still, such dramatic changes cannot be overlooked.
Methods A retrospective study was conducted on 468 patients who underwent ablation for CTI dependent typical AFL at a single institution between 2010 and 2019. Echocardiographic data were analyzed at baseline before ablation, and at early follow-up within 1-year postablation.
For instance, the average waiting time for an echocardiogram at Turin’s Molinette Hospital was 31 days in 2016 and an even longer 53 days for a Holter ECG. Prior to the new regulation, getting a consultation with a cardiologist or getting a needed diagnostic cardiology test often involved long waiting times.
A rapid echocardiogram was performed, revealing an ejection fraction of 20% with thinning of the anterior-apical walls. Although the patient reported experiencing mild pressure-like chest pain, there was suspicion among clinicians that this might be indicative of an older change. The initial troponin T level was measured at 30 ng/L.
Elevated troponins prompted an echocardiogram — which revealed an apical wall motion abnormality (WMA). We have addresssed this issue on a number of occasions ( See My Comment in the April 25, 2023 — July 21, 2019 — December 10, 2019 — and January 10, 2020 posts). Patient #1 in today's post did not get expert ECG interpretation.
Echocardiogram was obtained and showed mild LVH without regional wall motion abnormality. Rather than loss of both a J wave and S wave — there is a "slur" ( J-point equivalent ) in lead V2 of ECG #2 ( See My Comment in the November 14, 2019 post for illustration of T-QRS-D ). ng/mL and 0.10 ng/mL before returning to 0.05
Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. JACC 2019 Sep 10;74(10):1290-1300. The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region.
While awaiting transfer to the cath lab, STAT echocardiogram was performed and showed LVEF 30-35%, as well as anterior, inferior, and apical hypokinesis, and apical thrombus. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity.
See this case: what do you think the echocardiogram shows in this case? Am J Med 2019, 132(5):622-630. Now there is a paper published in 2019 that proves the point beyond doubt, though makes it clear that this pattern is associated with very high mortality. American Journal of Medicine 132(5):622-630; May 2019.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 That said — I illustrate HOW this RATIO is arrived at in Figure-2 , which I have adapted from the 3/16/2019 post in Life-In-The-Fast-Lane. Troponins gradually trended down from 0.19
Indeed, bedside Echocardiogram revealed severe left ventricular impairment of Takotsubo cardiomyopathy. Surawicz and Knilans report that intense catecholamine surge, or severe maladjustment of the autonomic nervous system, can manifest “cerebral T waves” in the absence of an acute intracranial process. potassium) were within normal parameter.
Get an emergent contrast echocardiogram. QTc's were 330 ms and 373 ms This is what I texted back: These look like they are a very pronounced case of Benign T-wave Inversion. I do not think this is acute occlusion myocardial infarction (OMI). These are reasons why it does not look like OMI: 1. flat ST segment in V4 2. huge R-wave in V4 3.
Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. She went to the cath lab and had a 100% Obtuse Marginal Occlusion (supplying the lateral and posterior wall) with TIMI-0 flow. A massive acute OMI.
Athena was developed in 2019 to create a partner network to improve the care continuum. The award-winning medical FHIR API even offers healthcare app developers the opportunity to create more solutions. Athena Cardiology EHR (Athenahealth) Another top contender for cardiology EHR is Athena Cardiology EHR.
Another way of imaging the heart is via a transesophageal echocardiogram. References: Mendirichaga et al, Evaluation of Cryptogenic stroke; American College of Cardiology 2019 The post Cryptogenic Stroke appeared first on Dr Sanjay Gupta Cardiologist.
Formal Echocardiogram: The estimated left ventricular ejection fraction is 58 %. We wrote this Editorial in the Journal of Electrocardiology in 2019. Because it reperfused on its own and because we intervened before it could re-occlude. Left ventricular hypertrophy concentric. Litell JM, Meyers HP, Smith SW.
Unfortunately there is no echocardiogram accessible because the patient checked himself out of the hospital in order to get back to his home state before it could be completed. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. To our knowledge, the patient did well.
I have ordered an echocardiogram which will be done today, after that patient can be discharged to home with follow-up in 2 to 3 months." Not all forms of idiopathic VT are predictable based on their ECG appearance ( Anderson et al, 2019 ). The echo was normal. Learning points 1.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Heart Rhythm, 15(9): 1394-1401. [7]
An echocardiogram was done. Kazmi et al have reported on a case in which chest trauma was transiently associated with development of a Brugada-1 ECG pattern ( J Am Coll Cardiol 73 [9-Supp-1], 2019 ). Is there also Brugada? Here is the result: The estimated left ventricular ejection fraction is 50 %. Right ventricular prominence.
Echocardiogram: Estimated left ventricular ejection fraction, lower limits of normal; 45-50%. M Y T HOUGHTS : I have previously reviewed my Systematic Approach to Rhythm Interpretation ( See My Comment in the October 16, 2019 post ). Tele Monitor: Normal sinus rhythm throughout, no ectopic atrial or ventricular beats.
After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." For more on T-QRS-D — Please see My Comment at the bottom of the page in the November 14, 2019 post in Dr. Smith's ECG Blog ).
When I heard she had not undergone immediate angiogram, my first question was, "Did she die?" == Comment by K EN G RAUER, MD ( 4/3/2019 ): == Insightful case presented by Dr. Smith — of an elderly woman with acute LAD OMI. Anyone can die of LAD occlusion, but especially the very elderly and especially if they are not reperfused.
Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
Later, he underwent a formal echocardiogram: Very severe left ventricular enlargement (LVED diameter 7.4 E CG # 2 in Figure-1 is from the October 16, 2019 post on Dr. Smith’s Blog. I review my S ystematic A pproach to Rhythm Interpretation in detail in My Comment to the October 16, 2019 post on Dr. Smith’s ECG Blog.
Despite apparently hearing the above history together with two diagnostic ECGs and a troponin compatible with OMI, the cardiologist thought the ECG represented pericarditis and recommended echocardiogram. Echocardiogram was finally performed five hours after the first diagnostic ECG. This far out, the benefit of PCI is very attenuated.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content