This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
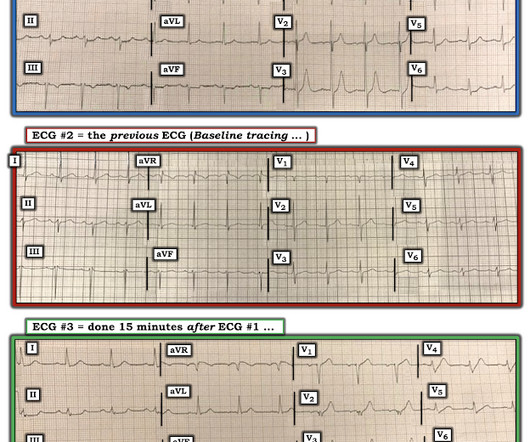
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Past medical history included diabetes and hypertension.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. From My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog: A subject well worth periodic review — is the concept of Terminal QRS Distortion ( T-QRS-D ).
Case submitted and written by Mazen El-Baba MD, with edits from Jesse McLaren and edits/comments by Smith and Grauer A 90-year old with a past medical history of atrial fibrillation, type-2 diabetes, hypertension, dyslipidemia, presented with acute onset chest/epigastric pain, nausea, and vomiting. Am J Med 2019, 132(5):622-630.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago. That was also my initial concern. No "baseline" ECG is available for comparison.
Written by Pendell Meyers, sent by Anonymous A man in his 50s with history of type 2 diabetes, HTN, and HLD presented with one day of off and on chest / upper abdominal pain. Some patients will not progress (or not as quickly) to obvious STEMI, as in this case. Vitals were within normal limits.
Higher troponin correlated with more history of heart failure, diabetes, and hypertension, as well as higher D-dimer, and nearly all inflammatory markers. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. Median age was 66.4
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. In today’s case the patient is suffering from diabetic ketoacidosis, which facilitates hydrogen ion shift into the cells in exchange for potassium. Elsevier-Saunders: Philadelphia, PA. [6].
Written by Pendell Meyers A woman in her 70s with diabetes, hypertension, and hyperlipidemia suddenly developed nausea, diaphoresis, and brief syncope while eating at a restaurant. This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. Serial troponins were negative.
Case 2: sent by Dr. James Alva A man in his 50s with diabetes, hypertension, and hyperlipidemia presented to the ED with chest pain and shortness of breath off and on over the past three days, with associated vomiting. There is also much STE in V3-V6, especially V4-V6, that must be considered to be STEMI. Peak troponin was 3.21
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chest pain. OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific. The patient was very agitated and could not hold still.
edits by Meyers A woman in her 60s with a history of chronic atrial fibrillation on Eliquis, ESRD on hemodialysis, type-II diabetes mellitus, prior CVA, hypertension, and hyperlipidemia presented to the emergency department with multiple complaints after missing dialysis. Is this inferor STEMI? Atrial Flutter with Inferior STEMI?
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chest pain. 2019 Apr;21(5):253-258. Written by Emre Aslanger. Emre is a new Editor of the Blog. He is an interventionalist in Turkey. 2019.09465.
Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia? And more cases, if you want, at this link. == My Comment, by K EN G RAUER, MD ( 3/2/2019 ): == The importance of this case lies in recognition of a number of findings, and the differential diagnoses that these findings should evoke.
C ASE F ollow- U p: I later learned the history in today's case which was that a middle-aged man with diabetes and hypertension who presented to the ED ( E mergency D epartment ) for abdominal pain that had awakened him from sleep. Figure-4: I've labeled KEY findings in today's ECG.
Written by Willy Frick A man in his mid 30s with type 1 diabetes presented with two days of midsternal and epigastric pain, described as both "sharp" and squeezing." The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI."
Written by Jesse McLaren An 80 year old patient with diabetes/hypertension/ cirrhosis had a recent increase in candesartan for their hypertension, and was also on spirolactone and nadolol. iv ) This 80-year old patient with known diabetes, hypertension and renal insufficiency has worsening renal function on this admission.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content