This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
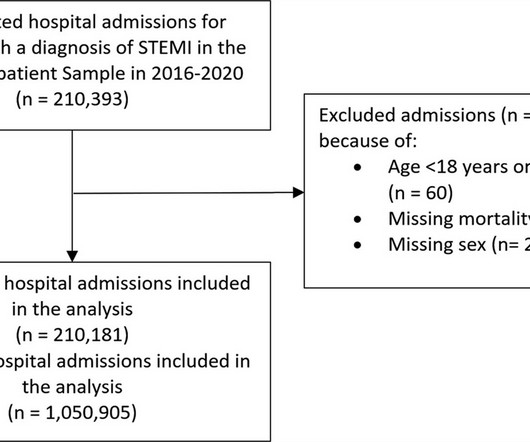
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% for patients admitted in 2016–2019 period. reduction in admissions in 2020.
Background Several studies have demonstrated that complete revascularisation improves clinical outcomes in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronarydisease. However, the optimal timing of non-culprit lesion revascularisation remains controversial.
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Registry data indicate that 6–11% of patients with acute MI have nonobstructive coronaryarteries.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. Studies of patients with coronaryarterydisease who developed arrhythmic storm with episodes of PMVT following MI — show arrhythmias indistinguishable from those reported in this case. The below ECG was recorded.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Incidence of an acute coronary occlusion.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronaryarterydisease, but there was spontaneous coronaryartery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronaryarterydisease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Registry data indicate that 6–11% of patients with acute MI have nonobstructive coronaryarteries.
Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. But the stuttering pain and sudden onset suggest acute coronary occlusion (Occlusion MI, or OMI). "ECG Cath lab activation by the ED and I agree with coronary angiography emergently." Result: no angiographically significant obstructive coronaryarterydisease.
He was taken emergently to the cardiac catheterization lab and found to have multi-vessel coronaryarterydisease with a near-occlusive culprit lesion in the RCA, possibly reperfused. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. J Electrocardiol 2013;46:240-8. Hypokalemia is frequently forgotten as a cause of ST depression. ST depression: is it ischemia?
Circumstances attending 100 sudden deaths from coronaryarterydisease with coroners necropsies. Prognostic implications of Doortoballoon time and onsettodoor time on mortality in patients with stsegmentelevation myocardial infarction treated with primary percutaneous coronary intervention. Heart , 37 (11), 11331143.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content