This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A common feedback I get is that people with existing coronaryarterydisease feel like it doesn’t apply to them. Arguably, applying the principles of prevention offers more bang for buck in the short term for people WITH coronaryarterydisease than those without coronaryarterydisease.
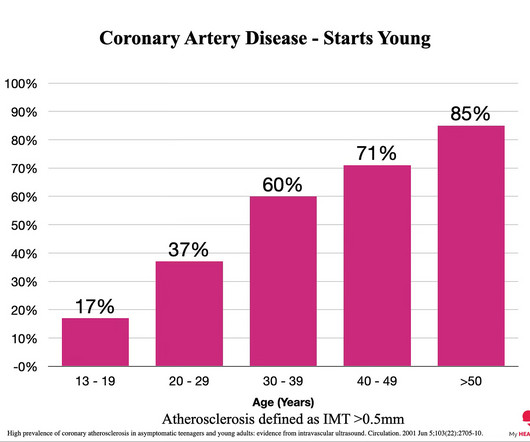
Everyone starts with no plaque in the coronaryarteries, but over a long enough time frame, everyone develops plaque in their coronaryarteries. By age 80, almost everyone will have evidence of advanced plaque in their coronaryarteries, as defined by a cardiac CT 1.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 4 In the U.S.
Angiogram No obstructive epicardial coronaryarterydisease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. hours All Hyperacute T-wave and ST Depression is resolved. Echo The estimated left ventricular ejection fraction is 56 %.
CT coronary angiography, in addition to a CT CAC, is arguably the best test for estimating whether someone has evidence of coronaryarterydisease and what that means for their near-term risk of a heart attack. Mixed Plaque - A combination of both calcified and NON-calcified plaque.
However, most adults will start to develop advanced plaque in their coronaryarteries early in life. By age 66, more than half of all females will have evidence of advanced plaque in their coronaryarteries, as seen on a CT calcium score. Adults: Fall 2019. Circulation. 2006 Jan 3;113(1):30-7.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch). The ST-T wave appearance in lead aVR can be anything when there is acute LMain occlusion.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronaryarterydisease (atherosclerosis/plaque) that might rupture and cause a heart attack. And the less plaque you have, the lower the risk of a heart attack.
This is supported by the over 1 million marathon participants worldwide in 2019. link] In older adults, reasons for death often include further cardiovascular issues such as coronaryarterydisease, increasing the susceptibility to risk of injury or death during high exertion activity.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronaryarterydisease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). It can only be seen by IVUS.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Incidence of an acute coronary occlusion. Am J Med 2019, 132(5):622-630. Incidence of an Acute Coronary Occlusion. American Journal of Medicine 132(5):622-630; May 2019.
Angiogram: Severe coronaryartery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronaryarterydisease. This would be the likely source of the VT. Figure-1: The 2 ECGs in this case ( See text ).
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo. Mechanisms of plaque formation and rupture. Coronaryplaque disruption.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content