This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
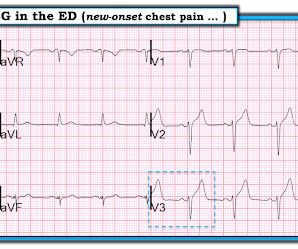
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. Litell JM, Meyers HP, Smith SW.
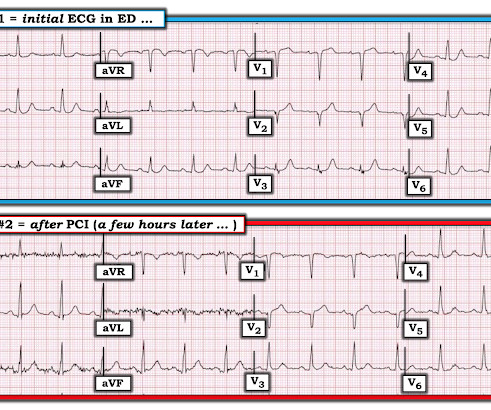
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Here is the post stent ECG: This is probably the amount of ST elevation (zero) that this patient has at baseline.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, Pericarditis would be even more unlikely in someone without chestpain.
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
A 50-something with no previous cardiac history and no risk factors presented to the ED with acute chestpain (pressure) that radiated to the left arm. It was stented with good results. An ECG was immediately recorded: Computer read: Normal ECG What do you think? There is ST depression in V1-V3.
Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent this case A 50-something man presented with acute chestpain. 100% proximal LAD successfully stented. Here is his ECG: As you can see, the computer called it completely normal What do you think? Defibrillated out of v fib in the cath lab.
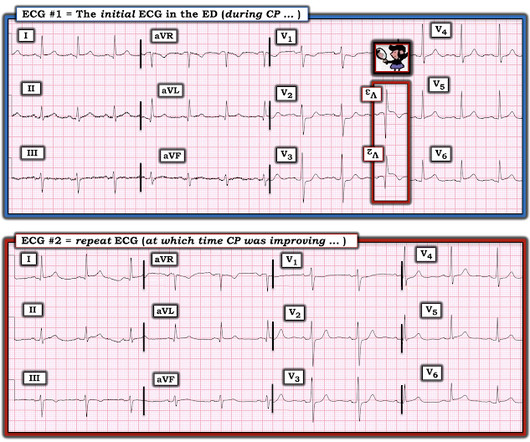
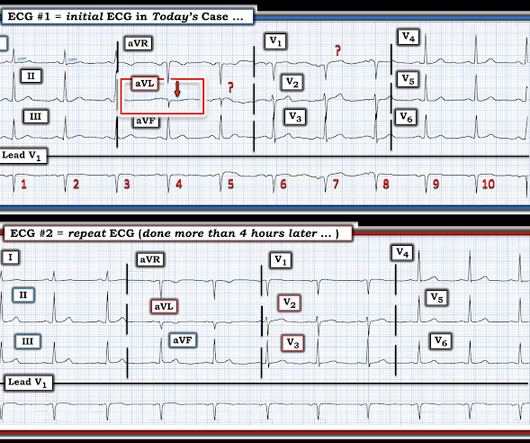
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. What do you think? Troponin I peaked at 18.323ng/L.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. It was stented. This was a large OMI.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. Although I do not see much difference between the ECGs, for some reason (perhaps ongoing pain or rising troponins) the case was reevaluated at this time and the decision was made to perform cath.
Troponin profile The patient underwent angiography and had a 90% thrombotic proximal LAD lesion that was stented. The patient is a 40-something year old man with new chestpain. In a patient with new chestpain — these T wave changes for beats labeled “ B ” in leads V1 , V2 and V3 constitute h yperacute T waves !
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The lesion was successfully stented, but it was unfortunately done after a significant myocardial loss. Anatol J Cardiol.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. It was stented. The patient had a p rior h istory of MI + stents. Time zero What do you think? There is inferior ST elevation. Is it normal variant? Is it ischemic (OMI)? Pericarditis? Compare with an old ECG.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She presented to the emergency department after a couple of days of chest discomfort. the most commonly overlooked arrhythmia ( See My Comment at the bottom of the page in the May 1, 2023 — and the November 12, 2019 post , among others ).
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented.
The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The chestpain was described as both sharp and pressure like. The culprit lesion was opened and stented. He is otherwise healthy.
A 40 something otherwise healthy man presented with substernal chestpain. They were stented. We wrote this Editorial in the Journal of Electrocardiology in 2019. It had occurred once 3 days prior and resolved without any medical visit. What do you think? This ECG is DIAGNOSTIC of acute LAD Occlusion. As per Dr.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. A mid-LAD culprit lesion was identified and stented. Below are two examples of this. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution.
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardial infarction presented to the ED with chestpain at 2343. It was treated with a drug eluting stent. It is awaiting FDA approval (but approved for 1.5 There is ST elevation in the inferior leads.
Written by Pendell Meyers An adult man presented with acute chestpain. He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). Acute chestpain, right bundle branch block, no STEMI criteria, and negative initial troponin.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019) Distinctive ECG patterns in healthy black adults. What do you think the prehospital ECG showed (with pain)? A stent was placed. See our article: Walsh, B.,
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. After stent placement: The vessel is now open with TIMI 3 flow, although it is diffusely diseased and the middle segment is ectatic.
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? It was opened and stented. The September 22, 2019 post — intermittent ST-T wave artifact. How do I know?
This is a very bold statement in a type 1 diabetic with very concerning sounding chestpain. The patient was treated with aspirin and a GI cocktail, which did not help the pain. The true AV groove LCx was "jailed" by the stent and appears occluded in the post PCI image. Here is an AP caudal view before and after PCI.
A 62 year old man with hyperlipidemia presented to a rural emergency department with 7 hours of 3/10 chestpain. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. In fact, much of what passes for EKG education can actually harm one's interpretation skills.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content