This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
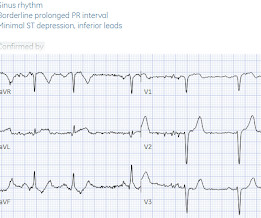
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. Clinical Cardiology 2019. Peak high sensitivity troponin T was 2,696 ng/L.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chestpain with diaphoresis, and called EMS. So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. What do you think?
Written by Jesse McLaren Four patients presented with chestpain. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
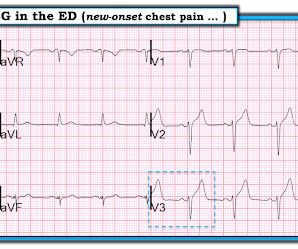
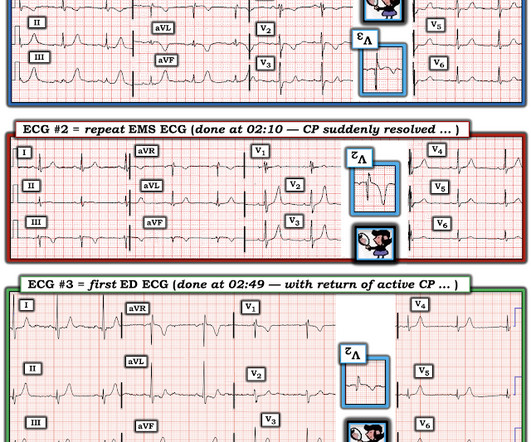
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. The ECG shows ST depression in lead V3.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chestpain and RBBB. Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. Do either, both, or neither have occlusion MI? Vitals were normal.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. And yet it still says "normal".
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD.
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Barely any STE, and thus not meeting STEMI criteria.
male was sitting at a work conference when he began having substernal chestpain with diaphoresis. The pain was 7 out of 10 when this ECG was recorded: The QTc = 375 What do you think? Since the threshold for "STEMI" is 2.0 mm, this ECG actually meets STEMI criteria. Since the threshold for "STEMI" is 2.0
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. But the stuttering pain and sudden onset suggest acute coronary occlusion (Occlusion MI, or OMI). No pericardial effusion on ultrasound."
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. This ECG was sent from South Asia.
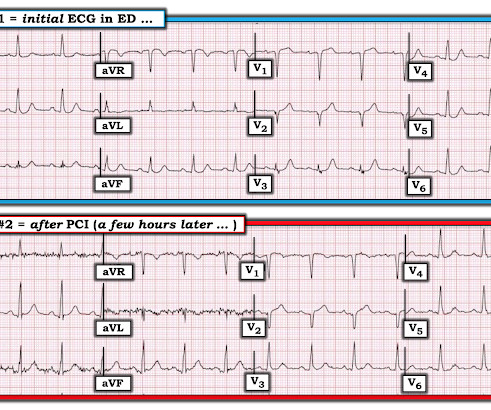
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1. Initial troponin was negative.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). But it does not meet STEMI criteria and it was not initially recognized.
Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent this case A 50-something man presented with acute chestpain. So there is definitely no STEMI, and the STE is normal. But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. mm in men over age 40.
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Anxiety is a common cause of chestpain with tachycardia.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion). The rhythm in ECG #1 is regular and supraventricular at a rate of ~75/minute. What is M INOCA?
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
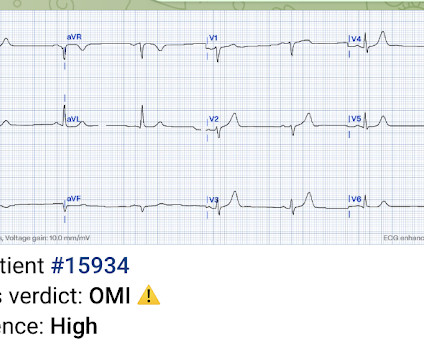
It is from a 50-something with chestpain: What do you think? This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. JAMA Intern Med 2019 9. Int J Cardiol 2013 2.
Discharge Diagnosis was STEMI (The STE did not meet "criteria," so "OMI" would be better, but "STEMI" is far better than what this could have been called: NonSTEMI) Quotes from a note written by a really fine and knowledgable physician: "12-lead EKG was obtained initial 1 at time zero. Chestpain is squeezing or tight in nature.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." Still does not meet STEMI criteria, but it is an obvious OMI And then another one became more obvious: Cath lab was activated and a 100% RCA occlusion was found. Sounds like reflux, right? Learning Points: 1.
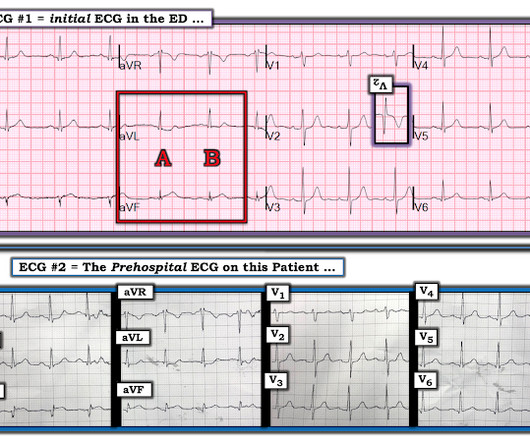
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chestpain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
Prompt cath is therefore advised if the post-ROSC shows an acute STEMI. I i llustrate the ECG finding of T-QRS-D below in Figure-3 , which I've excerpted from My Comment in the November 14, 2019 post in Dr. Smith's ECG Blog. To Emphasize: The phenomenon of T-QRS-D is not needed in today's case to recognize the acute STEMI.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. So it is very unclear to me whether or not "posterior STEMI" is actually a recognized entity under our current guidelines.
Algorithm: Veritas (on Mortara machines) The Queen gets it right Case 2 A middle-aged woman with chestpain and a "normal" ECG in triage. Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? Pain was resolving. The OMI was not seen and she arrested in triage.
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He wrote most of it and I (Smith) edited.
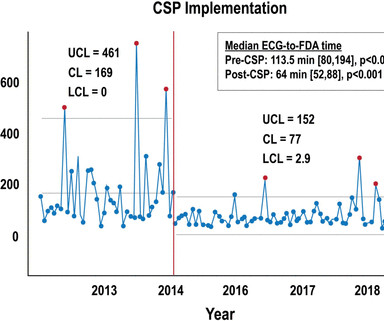
Methods This study included consecutive patients with iSTEMI treated with percutaneous coronary intervention (PCI) between 1 January 2011 and 15 July 2019 at a single, tertiary referral centre.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. This was a machine read STEMI positive OMI. We've highlighted a considerable number of acute RV MI cases in Dr. Smith's ECG Blog ( See the October 7, 2019 and May 10, 2024 posts , to name just two ).
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. N Engl J Med [Internet] 2019;Available from: [link] Should all patients with shockable arrest be taken to angiography regardless of STEMI or No STEMI?
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chestpain. Another similar case: Teenager with chestpain and slightly elevated troponin. 13, 2019 Dr. Smith post. 27, 2019 Dr. Smith post. What happens then? Pericarditis?
Written by Pendell Meyers A man in his early sixties with no significant medical history (including a "negative cardiac workup a few years ago" for unclear indication) called 911 for acute chestpain constantly for the past 5 hours. However, this patient has active chestpain, and thus this this is inferior-posterior OMI.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
Written by Pendell Meyers An elderly woman presented with acute onset chestpain and shortness of breath. There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. The delay between OMI and STEMI sometimes causes unacceptable loss of myocardium or worse.
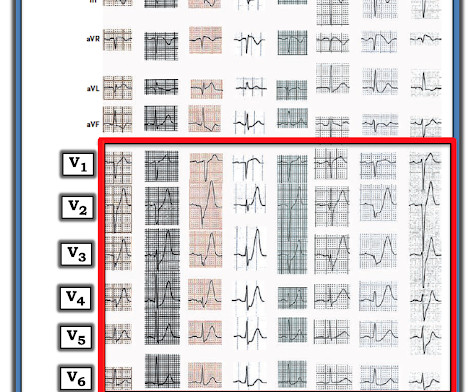
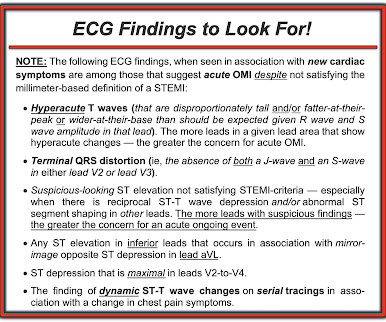
Of note — the patient reported a reduction in chestpain severity around the time ECG #2 was recorded. Figure-4: ECG findings to look for when your patient with new-onset cardiac symptoms does not manifest STEMI-criteria ST elevation on ECG.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content