This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. It is easy to say pericarditis in such a case.
A healthy 45-year-old female presented with chestpain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”.
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. This is OMI until proven otherwise.
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( From the information provided — I would not make the diagnosis of acute pericarditis. Figure-1: The initial ECG in today's case.
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. Pericarditis maybe." Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. Meyers' words — "is one of the rare ECGs that is actually specific for pericarditis".
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. Angiogram : "Acute onset chest pressure with diaphoresis." "ECG
Sent by Dan Singer MD, written by Meyers, edits by Smith A man in his late 30s presented with acute chestpain and normal vitals except tachycardia at about 115 bpm. Dr. Singer sent this to me with just the information: "~40 year old with acute chestpain". Acute pain?" -(Dr. I immediately responded: "cool fake!
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Assessment:" " Nonspecific ST elevation from V1-V4 , question of early repolarization versus pericarditis , question of acute current of injury and ? Pericarditis would be even more unlikely in someone without chestpain.
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chestpain. It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." Pericarditis? 13, 2019 Dr. Smith post.
Written by Pendell Meyers, with edits by Steve Smith A man in his early 40s with history of MI s/p PCI presented with bilateral anterior chestpain described as burning and belching with no radiation since last night starting around 11pm (roughly 11 hours ago). The patient was still with ongoing chestpain at the time ECG #1 was done.
In fact, there was no chestpain either. Pericarditis? If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. However, there is zero PR depression which would be VERY unusual in pericarditis. P.S.: Acute pericarditis may produce diffuse ST elevation.
Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? Expert ECG interpretation can often distinguish normal variant STE from OMI from pericarditis. Smith = “You diagnose acute pericarditis at your peril”. We will study this soon with our database.
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. Such an out-of-proportion STE is virtually never seen in pericarditis. 2019 Apr;21(5):253-258. Wait for the angiogram.
You do NOT see this in normal variant STE, nor in pericarditis. At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. Smith noted in his Learning Points about this Case that, “Many MIs do not have chestpain”.
They were recorded 12 minutes apart: "Hey Steve, 30-something with one week of chestpain, mostly right-sided, better with sitting up.": I learned more about the history: 30-something African American with 5-7days of sharp R-sided shoulder/scapula/chest discomfort, presented with sinus tachycardia. What do you think?
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. Pericarditis? A straight ST segment virtually never happens in inferior ST elevation that is NOT due to OMI (normal variant, pericarditis) 4. Time zero What do you think? There is inferior ST elevation.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. ST depression. Myocardial Contusion?
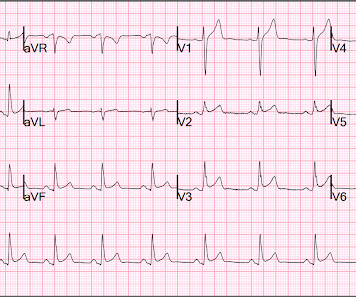
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” Neighboring Leads? — and the Rest of the ECG!
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. He reported 1.5
This is a very bold statement in a type 1 diabetic with very concerning sounding chestpain. The patient was treated with aspirin and a GI cocktail, which did not help the pain. The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI."
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content