This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I assumed it was a patient with acute chestpain. It was a man in his 30s with chestpain. Performance of Artificial Intelligence Powered ECG Analysis in Suspected ST-Segment Elevation MyocardialInfarction. This was sent to me from Sam Ghali ( @EM_Resus ) with no other information. What do you think, Steve?
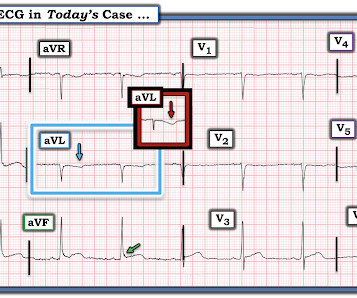
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). The ECG is diagnostic of occlusion myocardialinfarction (OMI). All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
Written by Pendell Meyers A man in his early 40s experienced acute onset chestpain. The chestpain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. Litell JM, Meyers HP, Smith SW.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? Pol Arch Intern Med. 2017;127:401–411. Circulation.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardialinfarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6. What do you think?
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." JACC 2019 Sep 10;74(10):1290-1300.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardialinfarction. Who needs the cath lab? Int J Cardiol Heart Vasc 2021 2. Aslanger et al. Lemkes et al.
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardialinfarction of any kind.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. JAMA Intern Med 2019 9. Int J Cardiol 2013 2.
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
Methods We prospectively included 1384 patients with LRHSs between March 2019 and March 2021. All the patients underwent NISI (involving myocardial perfusion imaging/stress echocardiography). The primary endpoints included cardiac death, non-fatal myocardialinfarction and unplanned coronary revascularisation.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chestpain and shortness of breath after finishing a 4-mile run. His symptoms of chestpain and shortness of breath were attributed to an asthma exacerbation during exercise.
== MY Comment by K EN G RAUER, MD ( 9/17/2020 ): == Todays patient is a previously healthy, 60-something year-old woman who presented with chestpain that began at a reception. We are indebted to Dr. Smith for developing Modified Smith-Sgarbossa Criteria for assessing ST-T wave changes in chestpain patients with LBBB.
The main heart attack symptoms assessed by the study were: Chestpain or discomfort Shortness of breath Pain or discomfort in arms or shoulders Feeling weak, lightheaded, or faint Jaw, neck, or back pain Reference Mahajan S, Valero-Elizondo J, Khera R, Desai NR, Blankstein R, Blaha MJ, Virani SS, Kash BA, Zoghbi WA, Krumholz HM, Nasir K.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
Cardiovascular diseases (CVDs) have been reported to occur in a significant number of patients diagnosed with coronavirus disease 2019 (COVID-19). Additionally, 2D transthoracic echocardiography (TTE), and myocardial injury serum biomarkers assays (creatine phosphokinase-MB [CPK-MB] and cardiac troponins [cTn]) were measured once.
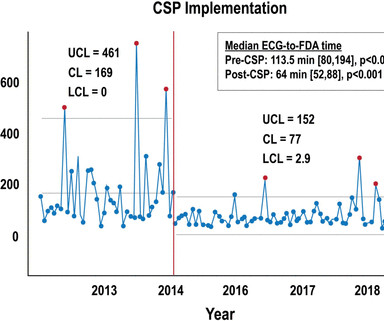
Background Patients who experience in-hospital ST-segment elevation myocardialinfarction (iSTEMI) represent a uniquely high-risk cohort owing to delays in diagnosis, prolonged time to reperfusion and increased mortality. Quality initiatives aimed at improving the care of this vulnerable, yet understudied population are needed.
However, data on whether a high-sensitivity HEART Pathway (hs-HP) are safe and effective is lacking.METHODS:An interrupted time series study was conducted at 5 North Carolina sites in 26 126 adult emergency department patients being investigated for possible acute coronary syndrome and without ST-segment–elevation myocardialinfarction.
He was asked multiple times about chestpain or dyspnea, but repeatedly denied any such symptoms. Patient denied chestpain on initial review of symptoms. Was now endorsing chestpain which began 30 minutes ago. Upon further questioning, he states that he has had intermittent chestpain since yesterday.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. I believe this is by far the most common outcome for this patient around the world in 2019. This ECG was recorded on arrival: What do you think? mm STE in V1 and 1.5-2.0
A 50 something-year-old man with a history of newly diagnosed hypertension and diabetes, for which he did not take any medication, presented a non-PCI-capable center with a vague, but central chestpain. The ECG in ER is shown below: ECG is still diagnostic but we are watching the natural course of myocardialinfarction here.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
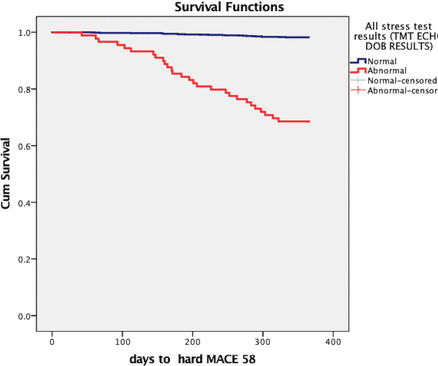
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization. Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. J Electrocardiol. 2017 Sep-Oct;50(5):561-569. doi: 10.1016/j.jelectrocard.2017.04.005.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Cardiac Troponin Changes to Distinguish Type 1 and Type 2 MyocardialInfarction and 180-Day Mortality Risk. At some point he returned with chestpain, and all these findings were put into place. Many MI do not have chestpain 4. The most common “non-chest-pain-equivalent” symptom is shortness of breath.
Terminal QRS distortion ( ie, the absence of both a J-wave and an S-wave in either lead V2 or lead V3 ) — SEE My Comment in the November 14, 2019 post for an illustration and description of T-QRS-D. The more leads in a given lead area that show hyperacute changes — the greater the concern for acute OMI.
They were recorded 12 minutes apart: "Hey Steve, 30-something with one week of chestpain, mostly right-sided, better with sitting up.": I do not think this is acute occlusion myocardialinfarction (OMI). This history of a week of constant chestpain is also much more suggestive of myocarditis.
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chestpain who was headed to an outside hospital (which happens to be a catheterization center).
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. V5-V6) of any amplitude, is specific for Occlusion MyocardialInfarction (vs. The patient was very agitated and could not hold still. Meyers, Bracey, Smith, et al.
Written by Pendell Meyers, few edits by Smith A man in his 60s with history of stroke and hypertension but no known heart disease presented with chestpain that started on the morning of presentation at around 8am. Here is his triage ECG when he presented at 1657: What do you think?
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. Am J Med 2019, 132(5):622-630. American Journal of Medicine 132(5):622-630; May 2019.
A 40 something otherwise healthy man presented with substernal chestpain. We wrote this Editorial in the Journal of Electrocardiology in 2019. To amplify remarks by Dr. Smith above — considering the clinical context (ie, new-onset substernal chestpain ) — no less than 9/12 leads in ECG #1 are clearly abnormal.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Below are two examples of this.
History : An extremely elderly patient who lived independently presented with acute "oppressive" chestpain 7/10 in severity that was not positional, pleuritic, or reproducible. Appearance of Abnormal Q Waves Early in the Course of Acute MyocardialInfarction: Implications for Efficacy of Thrombolytic Therapy.”
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Eur Heart J 2019 5.
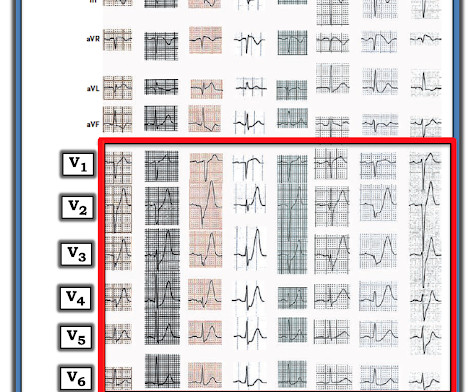
Written by Jesse McLaren Two patients presented with acute chestpain, and below are the precordial leads V1-6 for each. Hyperacute T waves can be a useful sign of occlusion myocardialinfarction if appropriately defined. Acad Emerg Med 2023 3. Smith, Meyers. Ann Emerg Med 2023 4. Meyers, Bracey et al.
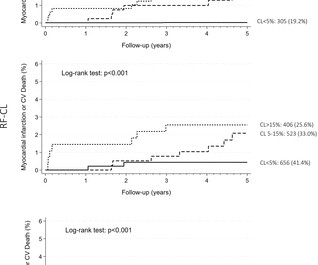
Compared to the 2019 European Society of Cardiology pretest probability (ESC-PTP) model, the aims were (1) to validate the RF-CL and CACS-CL models for identification of obstructive CAD and revascularisation, and (2) to investigate prognosis by CL thresholds. The endpoint was non-fatal myocardialinfarction or cardiovascular death.
Case A 76 year old man with chronic hypertension but no history of coronary disease or myocardialinfarction presented to the ED with chestpain at 2343. We've reviewed illustrative cases on this subject often ( See My Comment in the September 17, 2020 post and the April 7, 2019 post , among others ).
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. SanzRuiz, R., Solis, J., & link] Bai, J.,
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? The September 22, 2019 post — intermittent ST-T wave artifact. The August 26, 2019 post — baseline artifact.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content