This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sent by Magnus Nossen MD, written by Pendell Meyers A man in his 50s, previously healthy, developed acute chestpain. The primary care physician there evaluated this patient and deemed the chestpain to be due to gastrointestinal causes. Clinical Cardiology 2019. No troponins were measured!
Written by Magnus Nossen with Edits by Grauer and Smith The ECGs in today’s case are from 3 different patients all presenting with new-onset CP ( ChestPain ). In any case, the ECG is diagnostic of severe ischemia and probably OMI. All ECGs were recorded by EMS, and transferred to a PCI capable center for evaluation.
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chestpain. The patient is a young adult male with chestpain. The chestpain was described as pressure like and radiation to both arms and the jaw. How would you assess this ECG? What is your next step?
Written by Jesse McLaren Four patients presented with chestpain. Other signs of OMI that complement the ECG include new regional wall motion abnormalities and refractory ischemia References 1. 2019 ; 54 : 79 - 81. Hughes KE , Lewis SM , Katz L , Jones J. Acad Emerg Med. 2017 ; 24 ( 1 ): 120 - 124 2. Am J Emerg Med.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia.
A previously healthy middle-aged male presented shortly after the acute onset of chestpain very shortly before calling 911. On arrival, he was pain free: What do you think? Jerry Jones commented: "Any ST depression on the ECG of a patient with chestpain credible for ACS represents a reciprocal change until proved otherwise."
This is a previously healthy male teenager who was awoken by chestpain. The pain is described as located in the midsternal area, radiating to the right arm, described as 8-9/10 and worse with deep inspirations. In the evening, he became diaphoretic and complained of 9/10 continuous chestpain.
An elderly woman presented with chestpain that radiated to the back for several hours. The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. JAMA Intern Med 2019 9. Int J Cardiol 2013 2.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
He then went on to say: "40-something with chestpain for one hour. Burning pain subxiphoid and into throat." It does not usually represent subendocardial ischemia, but rather it is usually reciprocal ST depression, reciprocal to inferior ST elevation. (But Had episode of nausea and dizziness when it started.
Written and submitted by Ashley Mogul, with edits by Pendell Meyers and Steve Smith A man in his 40s with recent smoking cessation but otherwise no known past medical history presented due to chestpain since the previous evening. The pain has been constant and associated with vomiting and diaphoresis.
Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent this case A 50-something man presented with acute chestpain. It could at least say: "ST Elevation, consistent with normal variant," or "consistent with ischemia or normal variant," or "consistent with early repolarization." How do we do so?
A 50-something male who is healthy and active with no previous medical history presented with 5 hours of continuous worrisome chestpain. Chestpain with New LBBB: It helps to actually measure the ST/S ratio A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia The cath lab was activated.
2 days later This is a typical LVH pattern, without ischemia Patient underwent 4 vessel CABG. Upon questioning patient, he denies having any chestpain or chest tightness of any sort. Pericarditis would be even more unlikely in someone without chestpain. Chestpain is squeezing or tight in nature.
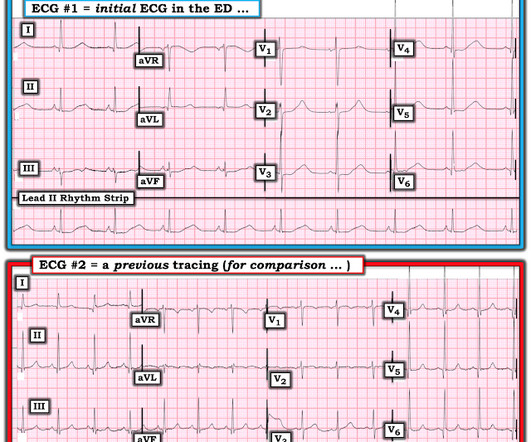
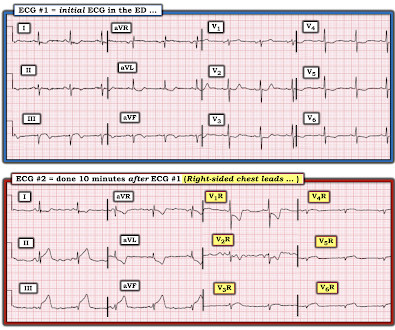
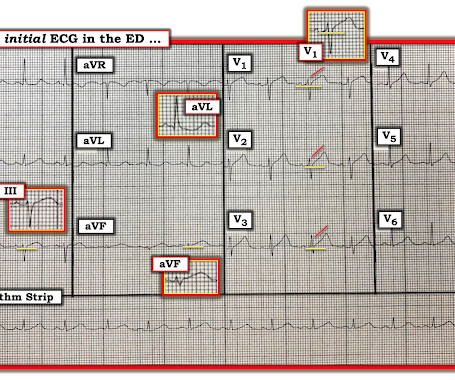
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
A 40-something woman with h/o obesity, hyperlipidemia, smoking, as well as cocaine and alcohol abuse presented with intermittent chestpain for 2-3 weeks that became constant in the last day. I illustrate use of a Systematic Approach to ECG Interpretation in My Comment at the bottom of the June 28, 2019 SSmith Post ).
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS.
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. Today's patient is a middle-aged woman who presented with low back pain, shortness of breath and marked hypertension — but no chestpain.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM Line: Today's patient presented with a 2-3 day history of chestpain and the ECG shown in Figure-1.
Written by Willy Frick A 50 year old man with no medical history presented with acute onset substernal chestpain. In this patient's case, the RV ischemia manifested as dramatic anterior hyperacute T waves. This degree of STE is a bit atypical for LAD ischemia. His ECG is shown below.
Context: a man in his 40s presented to the emergency department with 1 day of sudden onset chestpain. That said — I did not interpret these differences as the result of acute ischemia. I sent this to our group without information and Dr. Smith responded: "Not OMI. Pericarditis maybe."
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS.
A middle aged man had off and on chestpain for 2 weeks, then 2 hours of more severe and constant pain. Contrary to what Ken stated, the ST vector remains mostly posterior __ What about subendocardial ischemia? Similarly, STD in aVL is usually reciprocal to inferior ST elevation, not "lateral ischemia."
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Still, such dramatic changes cannot be overlooked.
But, in a patient who presents to the ED for new chestpain — seeing these subtle findings that are localized to leads V2- thru -V4 should at the least make you consider acute posterior OMI ( O cclusion-based MI ) — until you prove otherwise. To EMPHASIZE: These are subtle findings. What do YOU think?
Are you confident there is no ischemia? Primary VT , and the VT with tachycardia is causing ischemia with chest discomfort (supply-demand mismatch/type 2 MI)? Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Do you agree with this strategy?
The ECG in Figure-1 was obtained from a man in his mid-60s — who presented with new chestpain. The magnitude of ST-T wave change is maximal in lead V2 — with the insert in this lead showing a positive "Mirror" Test — that in this patient who presents with new chestpain, is diagnostic of acute posterior OMI — until proven otherwise.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Am J Med 2019, 132(5):622-630. Anything more on history?
Although the patient reported experiencing mild pressure-like chestpain, there was suspicion among clinicians that this might be indicative of an older change. The patient rapidly regained consciousness, reporting no residual pain. There is some ST-segment elevation in DII, DIII, aVF, V4-6.
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." Here is the patient's troponin I profile: These were interpreted as due to demand ischemia, or type II MI. ng/mL is seldom a result of demand ischemia (type 2 MI). First was 2.9
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chestpain.
or basilar ischemia. Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. EKG on arrival to the ED is shown below: What do you think? On my initial interpretation, the patient has normal sinus rhythm with a narrow QRS complex, and LVH.
She did not report any chestpain or pressure. She was brought to the Emergency Department and this ECG was recorded while she was still feeling nauseous but denied chestpain, shortness of breath, or other symptoms: What do you think? The morphology of STE is not diagnostic of being due to acute transmural ischemia.
A 40-something woman presented to the ED having had “heartburn” overnight and then worsening chestpain 1 hour prior to arrival. Resolution of pain, by itself, is not reliable enough to be certain of resolution of ischemia. the ischemia has truly resolved. This was sent by Cam Mosley, LSU-Baton Rouge Residency.
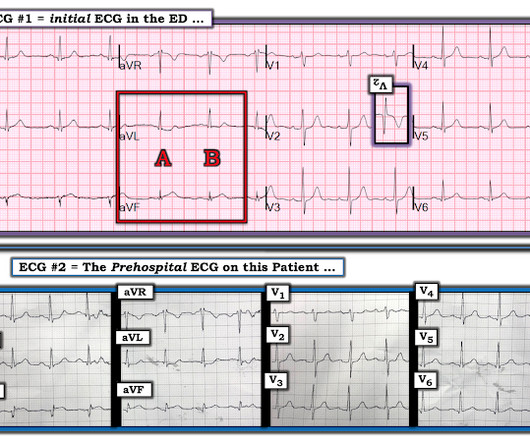
This patient's ischemia was so brief that it did not cause any myocardial stunning. The patient is a 40-something year old man with new chestpain. In a patient with new chestpain — these T wave changes for beats labeled “ B ” in leads V1 , V2 and V3 constitute h yperacute T waves ! The QTc is normal.
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chestpain. Does this mean that the ST depression in V3 represents "anterior" subendocardial ischemia, and not posterior OMI? non-occlusive ischemia) 2.
Although as a general rule, there should be no ST elevation in RBBB in the absence of ischemia, there sometimes is ST elevation that looks like this. If the ECG findings are truly new compared to a baseline (unavailable), this could suggest persistent ECG findings of ischemia, meaning poor downstream perfusion ("no reflow" phenomenon).
Written by Pendell Meyers A male in his early 50s presented with waxing and waning chestpain starting at rest. He had multiple cardiovascular risk factors and the EM physician strongly suspected ACS. Here is his initial ECG: What do you think? mm), neither of it's neighbors have enough STE to meet criteria (V1 is close at 0.5
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
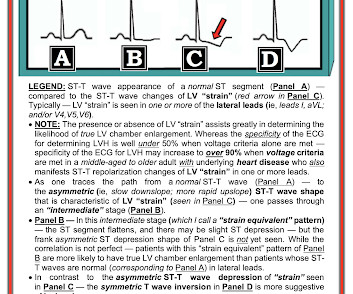
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. Hypokalemia c.
So this relatively long QT interval is NOT due to ischemia but may be a result of CO Toxicity. Read more about CO poisoning and cardiac ischemia here (ECG is pasted below): What is the treatment for this subendocardial ischemia? See this case of an awake patient without chestpain but with a CO level of 34%: CO poisoning.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content