This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Healthy male under 25 years old with a pretty good story for acute onset crushing chestpain relieved with nitro. Cath lab activation by the ED and I agree with coronary angiography emergently." Result: no angiographically significant obstructive coronaryarterydisease. What do you think? Medical Rx.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
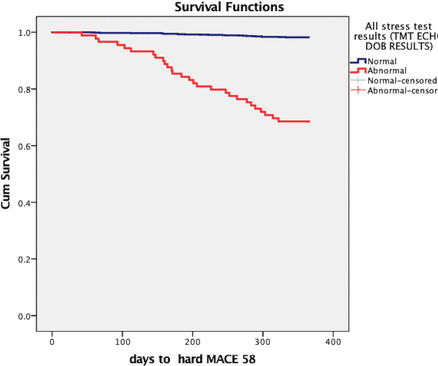
Methods We prospectively included 1384 patients with LRHSs between March 2019 and March 2021. The primary endpoints included cardiac death, non-fatal myocardial infarction and unplanned coronary revascularisation. All the patients underwent NISI (involving myocardial perfusion imaging/stress echocardiography).
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronaryarterydisease with supply/demand mismatch).
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronaryarterydisease and myocardial infarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
CT coronary angiography, in addition to a CT CAC, is arguably the best test for estimating whether someone has evidence of coronaryarterydisease and what that means for their near-term risk of a heart attack. This article is part 2 of a series on cardiac CT. I would say yes. For very good reason. And it matters.
63 years old Afsar Khan resident of Karwan, Hyderabad had been having coronaryarterydisease and chestpain on exertion for about a year. In November 2019, he underwent CT coronary angiography which showed blocks in all 3 coronaryarteries of the heart. He was still corona negative.
I think especially with the recent changes in guidelines and the recommendation to use CT for screening of coronaryarterydisease, we expect to see this trend really impact the way CT is used in the future.” “The CT procedural mix is evolving, and cardiac CT is starting to account for a large proportion of that.
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
A 70-something female with no previous cardiac history presented with acute chestpain. She awoke from sleep last night around 4:45 AM (3 hours prior to arrival) with pain that originated in her mid back. She stated the pain was achy/crampy. Over the course of the next hour, this pain turned into a pressure in her chest.
Preliminary findings documented in the cath lab were “Anterior STEMI and no significant coronaryarterydisease.” (!!!) Not a STEMI: Reasons I did not think ECG #1 represented an acute STEMI — included the following: There was no history of chestpain. ng/mL and 0.10 ng/mL before returning to 0.05
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. I believe this is by far the most common outcome for this patient around the world in 2019. European Heart Journal 2019. This is technically a STEMI, with 1.5
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. Incidence of an acute coronary occlusion. Am J Med 2019, 132(5):622-630. link] Harhash AA et al.
Share Let’s first state our goal when we are in the business of ‘Heart Disease Prevention’: To delay the onset of coronaryarterydisease (atherosclerosis/plaque) that might rupture and cause a heart attack. 2019 Sep 24;74(12):1582-1593. Not any more. Here’s why. J Am Coll Cardiol.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronaryarterydisease? Reference: Knotts RJ , Wilson JM, Kim E, Huang HD, Birnbaum Y. J Electrocardiol 2013;46:240-8. Hypokalemia is frequently forgotten as a cause of ST depression. You probably think it is left main.
Angiogram: Severe coronaryartery calcification Moderate to severe distal small vessel disease mainly seen in RPL1, 2 Otherwise, Mild plaque, no angiographically significant obstructive coronaryarterydisease. Figure-1: The 2 ECGs in this case ( See text ).
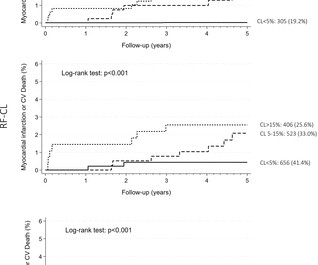
Objectives The risk factor-weighted and coronaryartery calcium score-weighted clinical likelihood (RF-CL and CACS-CL, respectively) models improve discrimination of patients with suspected obstructive coronaryarterydisease (CAD). However, external validation is warranted.
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. In my opinion, the ECG changes and hemodynamic collapse seem out of proportion to the observed/suspected coronary pathology. Circumstances attending 100 sudden deaths from coronaryarterydisease with coroners necropsies.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content