This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. It should be kept in mind that on occasions, beta-one agonist can result in increased ventricular ectopy e.g., in severe myocardial ischemia (by increasing myocardial demand), or sometimes with congenital long-QT syndrome.
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. 2] Here there is no posterior ST elevation, but the anterior ST depression is also less—so it is dynamic, confirming acute ischemia. What do you think? But it is still STEMI negative.
See this case, where a patient with BTWI morphology and dramatic EKG changes within minutes is diagnosed with myocarditis: [link] com/2019/07/what-does-this- ecg-with-significant-st.html EKG 3 also has a saddleback morphology in V2, which is only rarely due to OMI. Still, such dramatic changes cannot be overlooked.
Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Ischemia b. ST depression: is it ischemia? In my experience, Ive seen U waves not only with low K+/low Mg++ but also in patients with bradycardia, LVH, and sometimes in normal subjects.
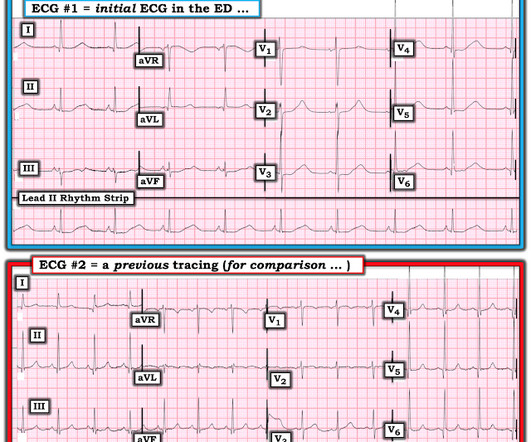
Thus, the long QU was probably all due to hypokalemia. == MY Comment by K EN G RAUER, MD ( 12/18/2019 ): == We have seen this picture that appears in the initial ECG in this case ( = E CG # 1 in Figure-1 ) more than a few times before on Dr. Smiths ECG Blog. Here it is: Normalized. Figure-1: The first 2 ECGs shown in this case ( See text ).
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. It is prudent to treat the other conditions, get the heart rate controlled, and repeat the ECG.
No more abnormal U-waves == MY Comment, by K EN G RAUER, MD ( 11/18/2019 ): == LOTS of great points regarding use of the ECG in association with electrolyte abnormalities. U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. N OTE # 1 — U waves are not specific for hypokalemia!
For coronary anatomy, see here: [link] This is the post intervention ECG: All ST Elevation is gone (more proof that it was all a result of ischemia) Formal Echo: Normal estimated left ventricular ejection fraction - 55%. This is sinus bradycardia. More likely, these T waves probably reflect ischemia of uncertain age.
IF the Patient is Younger and Athletic: The mechanism of AFib in younger, athletic individuals is often heavily influenced by increased vagal tone ( Rao and Shipon — ACC, 2019 — and — Calvo et al — Br J Sports Med, 2012 ). Baseline bradycardia in endurance athletes limits the use of ß-blockers.
These include ( among others ) — acute febrile illness — variations in autonomic tone — hypothermia — ischemia-infarction — malignant arrhythmias — cardiac arrest — and especially Hyperkalemia. Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
The patient later settled into sinus bradycardia. He was started on amiodarone and had no more events. Next day, the cardiologists were convinced (I think correctly) that this was SVT with aberrancy that was triggered by DKA.
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). What do you think?
There is no definite evidence of acute ischemia. (ie, Simply stated — t he patient was having recurrent PMVT without Q Tc prolongation, and without evidence of ongoing transmural ischemia. ( Some residual ischemia in the infarct border might still be present. Both episodes are initiated by an "R-on-T" phenomenon.
A prior ECG was available for comparison: Normal One might be tempted to interpret the ST depression as ischemia, but as Smith says, "when the QT is impossibly long, think of hypokalemia and a U-wave rather than T-wave." QUESTION #2: If it were not for the markedly prolonged QTc — Wouldn't ECG #1 look like diffuse subendocardial ischemia?
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. Bradycardia. Hypothermia.
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
Heart Rhythm, 15(10), e73-e189. -- Comment by K EN G RAUER, MD ( 1/30/2019 ): -- Superb presentation and discussion by Dr. Alexandra Schick ( with edits by Dr. Smith ) of an elderly woman who was seen in the ED for altered mental status, hyperthermia, and the initial ECG shown above. Heart Rhythm, 15(9): 1394-1401. [7]
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. It is possible there is microvascular dysfunction producing residual transmural ischemia. He told the patient this horrible news. The other point in favor of RCA is junctional rhythm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content