This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case An 82 year old man with a history of hypertension presented to the ED with chestpain at 1211. He described his chestpain as pleuritic and reported that it started the day prior while swinging a golf club. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive.
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. The patient in question presented with new-onset chestpain — and was from South(east) Asia. Bradycardia.
A 40-something woman with h/o obesity, hyperlipidemia, smoking, as well as cocaine and alcohol abuse presented with intermittent chestpain for 2-3 weeks that became constant in the last day. I illustrate use of a Systematic Approach to ECG Interpretation in My Comment at the bottom of the June 28, 2019 SSmith Post ).
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chestpain. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. Written By Magnus Nossen — with edits by Ken Grauer and Smith. The below ECG was recorded.
He did not have chestpain. Chestpain in high risk patient. Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Here is his triage ECG: What do you think? Is it STEMI? What is going on here?
He arrived to the ED by helicopter at 1507, about three hours after the start of his chestpain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chestpain around 1500 while eating. Still, such dramatic changes cannot be overlooked.
This fantastic case and post was written by Jesse McLaren (@ECGcases), edited by Smith Case You’re shown an ECG from a patient in the waiting room with chestpain. Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al.
Although in the context of chestpain such ST depression would be all but diagnostic of posterior OMI, one should make no conclusions in such an unusual case. In all leads, there is a 2nd wave after the initial QRS. This is an Osborn wave. I have not found any previous report of Osborn waves in RBBB.
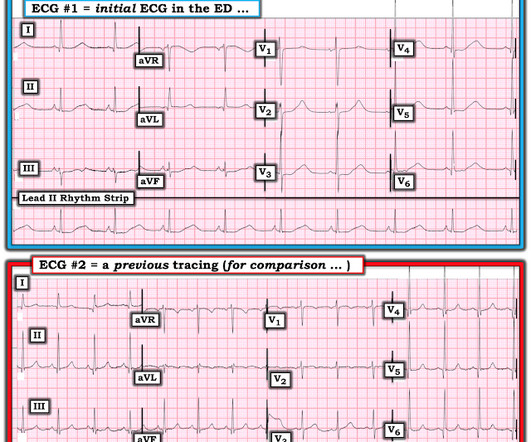
60-something with h/o MI and stents presented with chestpain radiating to the back and nausea/vomiting. Record serial ECGs. == Comment by K EN G RAUER, MD ( 6/28/2019 ): == I like this case because it provides an excellent example of how to use c omparison t racings in a patient with a prior history of coronary disease.
If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise. CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
Palpitations in a Young Healthy Male A pathognomonic ECG you should recognize instantly A middle-aged man with severe syncope, diffuse weakness Chestpain and Diffuse ST depression, with STE in aVR. You probably think it is left main. Are These Wellens' Waves?? ST depression: is it ischemia? No, hypokalemia.
No more abnormal U-waves == MY Comment, by K EN G RAUER, MD ( 11/18/2019 ): == LOTS of great points regarding use of the ECG in association with electrolyte abnormalities. This is often quite challenging to recognize — but the finding of negative U waves in a patient with chestpain is highly suggestive of ischemia !
She did notice something slightly wrong subjectively, but had no palpitations, chestpain, or SOB, or any other symptom. Baseline bradycardia in endurance athletes limits the use of ß-blockers. Ballatore et al — Medicina (Kaunas) 55(8): 497, 2019 — and — Page et al — Circulation 107:1141-1145, 2003 ).
It was from a patient with chestpain: Note the obvious Brugada pattern. The elevated troponin was attributed to either type 2 MI or to non-MI acute myocardial injury. There is no further workup at this time. Smith: Here is a case that was just texted to me today from a former resident. This patient ruled out for MI.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. Sinus bradycardia.” paramedic transportation to the ED as “chestpain, STEMI negative” 2.
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If The patient denied any chestpain whatsoever, and a troponin at zero and 2 hours were both undetectable. Annals of Noninvasive Electrocardiology 2019. 8, 2019 ) — ( Jan. 30, 2019 ) — many others.
days of chestpain that started as substernal and crushing in nature awakening him from sleep and occasionally traveling to right side of neck. The pain was described as constant, worse with deep inspiration and physical activity, sometimes sharp. He reported 1.5
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chestpain. A post-cath EKG was recorded at 0719: The computer interpretation read Sinus bradycardia, otherwise normal ECG. He had an EKG recorded right away.
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. He told the patient this horrible news.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content