This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. As described above by Dr. Smith Pacing in today's case is an effective intervention as doing so prevents the bradycardia and pauses that are likely to precipitate additional episodes of Torsades de Pointes. (
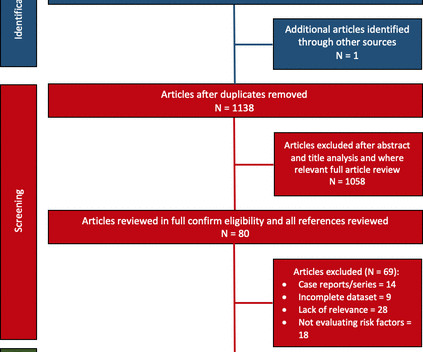
Objective We conducted a systematic review evaluating AF burden and bradycardia requiring permanent pacemaker (PPM) implantation and report any predictive risk factors identified. Methods We conducted a literature search on studies in adults with FD published from inception to July 2019. Age was associated with AF (OR 1.05–1.20
Both of these features make inferior + RV MI by far the most likely ( Pseudoanteroseptal MI is another name for this ) There is also sinus bradycardia and t he patient is in shock with hypotension. A narrow complex bradycardia without any P-waves is also likely to respond to atropine, as it may be a junctional rhythm.
Altered Mental Status, Bradycardia == MY Comment , by K EN G RAUER, MD ( 2/2 /2024 ): == Dr. Meyers began today’s case with the clinical challenge of asking you to identify the underlying cause of ECG #2. -- Read this ECG -- Osborn Waves and Hypothermia (this is the "Figure" above) What does LBBB look like in severe hypothermia?
There was no evidence bradycardia leading up to the runs of PMVT ( as tends to occur with Torsades ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
From March to July 2019, participants were asked to contact the study team for any irregular heart rate (HR) notification. Of 59 participants who sent at least 1 EKG, 52 (88.1%) were in sinus rhythm, 3 (5.1%) AF, 2 (3.4%) indeterminate, and 2 (3.4%) sinus bradycardia. 2 contacted their PCPs and were diagnosed with AF.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
Figure-1: Reasons for the varied ECG presentation of acute LMain occlusion — excerpted from Dr. Smith’s 8/9/2019 post ( This Table from My Comment in the January 16, 2020 post ). As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ).
He suffered from symptomatic bradycardia and falls for over a month and was seen by another cardiologist specifically for presyncope, and still the problem went unrecognized despite ongoing ECG evidence of pacemaker malfunction, and imaging proving lead dislodgement.
The November 12, 2019 post in Dr. Smith's ECG Blog — in which I review my approach to a Regular SVT rhythm. The August 17, 2020 post by me in Dr. Smith's ECG Blog — in which I review the phenomenon of Bradycardia-dependent BBB ( sometimes called "Phase 4" or "paradoxical" block ). ECG Blog #242 — Reviews rate -related BBB.
Syncope and Bradycardia Syncope in a 20-something woman Long QT: Do not trust the computerized QT interval when the QT is long An Alcoholic Patient with Syncope Cardiac Arrest. Is it STEMI? Chest pain in high risk patient. Are these Hyperacute T-waves? What is going on here?
Osborn waves have been reported with hypercalcemia, brain injury, subarachnoid hemorrhage, Brugada syndrome, cardiac arrest from VFib — and — severe, acute ischemia resulting in acute MI ( See My Comment in the November 22, 2019 post on Dr. Smith’s Blog ). Rituparna et al — as well as Chauhan and Brahma ( Int.
See this case, where a patient with BTWI morphology and dramatic EKG changes within minutes is diagnosed with myocarditis: [link] com/2019/07/what-does-this- ecg-with-significant-st.html EKG 3 also has a saddleback morphology in V2, which is only rarely due to OMI. Still, such dramatic changes cannot be overlooked.
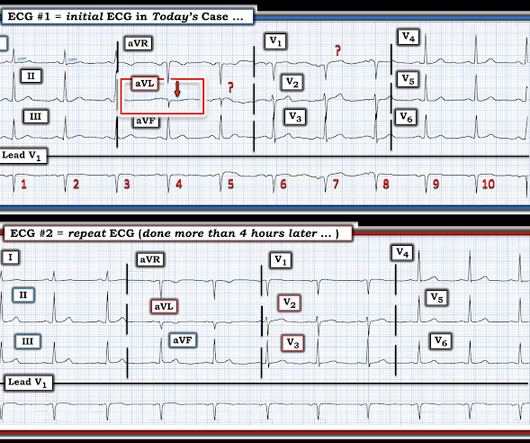
Thus, the long QU was probably all due to hypokalemia. == MY Comment by K EN G RAUER, MD ( 12/18/2019 ): == We have seen this picture that appears in the initial ECG in this case ( = E CG # 1 in Figure-1 ) more than a few times before on Dr. Smiths ECG Blog. Here it is: Normalized. Figure-1: The first 2 ECGs shown in this case ( See text ).
Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. A troponin T was drawn at 1229 and resulted slightly elevated at 23 ng/L (URL for men in this assay is 15 ng/L). The ED provider ordered a coronary CT scan to assess the patient for CAD.
Sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Int J Cardiol 2019 2. -- Meyers HP, Bracey, Smith et al. J Electrocardiol 2019 6. -- Amsterdam EA, Wenger NK, Brindis RG, et al. What do you think? Ischemic ST depression maximal in V1-V4 (vs.
IF the Patient is Younger and Athletic: The mechanism of AFib in younger, athletic individuals is often heavily influenced by increased vagal tone ( Rao and Shipon — ACC, 2019 — and — Calvo et al — Br J Sports Med, 2012 ). Baseline bradycardia in endurance athletes limits the use of ß-blockers.
No more abnormal U-waves == MY Comment, by K EN G RAUER, MD ( 11/18/2019 ): == LOTS of great points regarding use of the ECG in association with electrolyte abnormalities. U waves may also be found in patients with LVH and/or bradycardia , or occasionally as a normal variant. N OTE # 1 — U waves are not specific for hypokalemia!
Whatever today's rhythm turns out to be — the "good news" is that the bradycardia and degree of AV block is likely to improve as soon as there is reperfusion of the "culprit" artery ( Therefore need for prompt cath with PCI ). Smith’s ECG Blog with 20-minute video talk by Dr. Meyers on The O MI M anifesto.
Adenosine is safe in VT and may be useful in making the diagnosis. == MY Comment by K EN G RAUER, MD ( 12/23/2019 ): == It is ALWAYS great to welcome the contributions to Dr. Smith’s ECG Blog from Dr. Brooks Walsh — a highly skilled clinician + good friend and colleague who always stimulates conversation on important emergency medicine topics.
And more cases, if you want, at this link. == My Comment, by K EN G RAUER, MD ( 3/2/2019 ): == The importance of this case lies in recognition of a number of findings, and the differential diagnoses that these findings should evoke. Biphasic T-waves in a Middle-Aged Male with Vomiting Diabetic Ketoacidosis: is there hypokalemia?
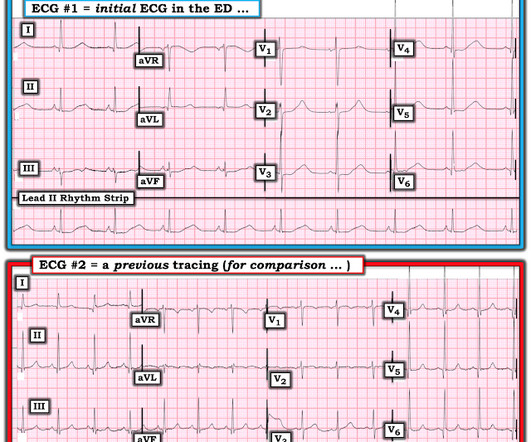
Record serial ECGs. == Comment by K EN G RAUER, MD ( 6/28/2019 ): == I like this case because it provides an excellent example of how to use c omparison t racings in a patient with a prior history of coronary disease. This is sinus bradycardia. Compare with an old ECG. The QRS is narrow. There is no chamber enlargement.
Heart Rhythm, 15(10), e73-e189. -- Comment by K EN G RAUER, MD ( 1/30/2019 ): -- Superb presentation and discussion by Dr. Alexandra Schick ( with edits by Dr. Smith ) of an elderly woman who was seen in the ED for altered mental status, hyperthermia, and the initial ECG shown above. Heart Rhythm, 15(9): 1394-1401. [7]
Kazmi et al have reported on a case in which chest trauma was transiently associated with development of a Brugada-1 ECG pattern ( J Am Coll Cardiol 73 [9-Supp-1], 2019 ). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). Sinus Tachycardia ( common in any trauma patient. ).
With a T ype 2 M I , d espite no acute coronary atherothrombosis — there will be positive Troponin with either new cardiac chest pain — and / or new ischemic ST-T wave ECG changes — and / or new Q waves on ECG — and / or objective demonstration of new wall motion abnormality.
The patient later settled into sinus bradycardia. He was started on amiodarone and had no more events. Next day, the cardiologists were convinced (I think correctly) that this was SVT with aberrancy that was triggered by DKA.
There’s sinus bradycardia, normal conduction, normal axis, delayed R wave progression, and normal voltages. The patient has a history of CABG so some of these changes could be old, but with ongoing chest pain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. Sinus bradycardia.”
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If Annals of Noninvasive Electrocardiology 2019. 8, 2019 ) — ( Jan. 30, 2019 ) — many others. EP study to further risk stratify her is recommended, with ICD placement depending on the results.
A repeat ECG was performed as adult cardiology was asked to evaluate the patient for emerget PCI: Sinus bradycardia with persistent elevation in the inferior leads with reciprocal depression in aVL Patient was taken to cath lab with adult cardiology which revealed normal coronary arteries without evidence of occlusion MI.
Theres sinus bradycardia, borderline PR interval, narrow QRS; normal axis/R wave progression; low precordial voltages, and subtle peaked T waves (most obvious in V2, but all T waves are symmetric with a narrow base). Theres no prior ECG to compare - but the bradycardia, prolonged PR and peaked T waves could all be from hyperkalemia.
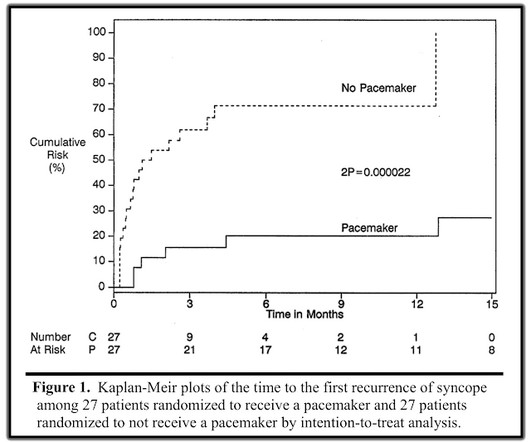
Perhaps because the bradycardia in vasovagal syncope is only one part of the autonomic response. Phase 4 block is also referred to as "bradycardia dependent block." A stunning result. One of many examples in medical history that remind us of the importance of blinding in clinical trials. Why was there no benefit?
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). He told the patient this horrible news.
As I've emphasized in the February 10, 2025 and March 19, 2019 posts hyperkalemia and hypocalcemia often occur together, and often produce a readily identifiable pattern of flat ST segments ending in peaked T waves that we see in today's case.
A post-cath EKG was recorded at 0719: The computer interpretation read Sinus bradycardia, otherwise normal ECG. This EKG was again called normal by both the computer and the overreading physician, although in the context of the previous two tracings, this finding suggests re-occlusion of the culprit artery. The troponin peaked at 0.4
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content