This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
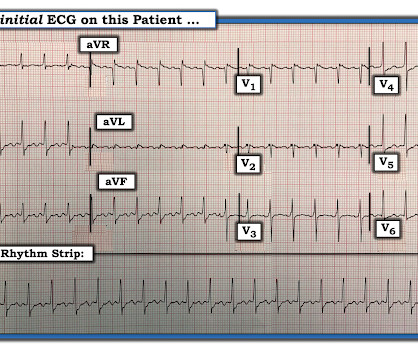
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. The ECG was interpreted as showing atrialflutter with 2:1 conduction. Answer : The ECG above shows a regular wide complex tachycardia. The heart rate could be compatible with that of a 2:1 conducted atrialflutter.
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? Are flutter waves hidden within the QRS and T waves? However, until such time that we know for certain — I think it best to simply describe what we see: PEARL # 1: Realize that for any tachycardia — there are 6 Parameters that need to be assessed. s in Figure-2 ).
Primary endpoint was the incidence of patients with new onset supraventricular arrhythmia (AF, atrialflutter or any supraventricular tachycardia) lasting >30s, post PFO closure.ResultsA total of 59 patients met the inclusion criteria.
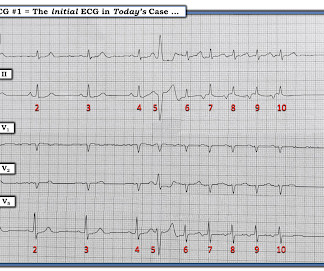
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
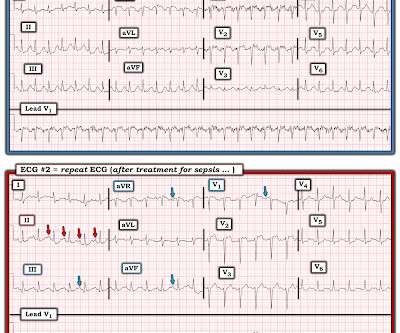
RBBB is no longer seen after conversion to sinus rhythm — which supports our suspicion that the intermittent RBBB conduction seen every-other-beat during the tachycardia ( in Figure-1 ) was rate-related. Note that QRS morphology after conversion to sinus rhythm is very similar to QRS morphology of odd-numbered beats during the tachycardia.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. They are flutter waves, and the rhythm is 2:1 atrialflutter.
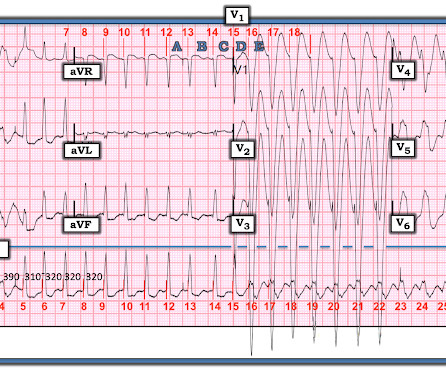
Are the wide complexes due to a supraventricular rhythm (AVNRT or Atrialflutter or atrial fib) with aberrancy? Or are they due to ventricular tachycardia (VT). The rhythm alternates between a wide complex (first 4 beats, and beats 16-28) and narrow complex (beats 5-15). There are no P-waves. Sinus P waves are absent.
The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. There are 5 other rhythms that are irregularly irregular , though atrial fibrillation is by far the most common: 1. Multifocal AtrialTachycardia 2. IJC Heart and Vasculature 25(2019). Sinus with multifocal PACs 3.
By this definition, a variety of rhythms may qualify as “SVTs” — including sinus tachycardia, atrialflutter or fibrillation, MAT, AVRT/AVNRT, among others. Why Isn’t this a Run of AtrialTachycardia? — ECG Blog #138 — AFlutter vs AtrialTachycardia.
== MY Comment by K EN G RAUER, MD ( 11/12/2019 ): == My appreciation to Kenneth Khoo for this case. M y A pproach to this R hythm : I reviewed the basics for rhythm interpretation in the October 16, 2019 Case from Dr. Smith’s ECG Blog. This patient was hemodynamically stable. What do YOU think the rhythm is?
PEARL # 3: AtrialFlutter with 1:1 AV conduction is rare! Since the rate of atrial activity with flutter in adults is most often very close to 300 /minute ( ie, usual range for atrial activity ~250-350/minute ) — AFlutter with 2:1 AV conduction typically results in a regular ventricular rate of ~140-160/minute.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Jimenez and Ali co-founded AccurKardia in 2019 with a vision for unlocking the value of the ECG signal, and the company currently markets one of the few FDA-cleared solutions for automated ECG interpretation and arrhythmia detection.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. There is a large peaked P-wave in lead II (right atrial enlargement) There is left axis deviation consistent with left anterior fascicular block. See my quick review of atrialtachycardia below) The tachycardia spontaneously resolved.
2** Furthermore, the primary effectiveness endpoint (PEE) of acute pulmonary vein isolation and 12-month freedom from atrial arrhythmia recurrence (AF, AtrialTachycardia, or AtrialFlutter) was 75.6%. 2019; 7[1]:110-118. iii] The study reported a low fluoroscopy time of 7.8 EMJ Cardiol. Clin Epidemiol.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content