This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
The 2019 ESC Guidelines for the management of patients with supraventricular tachycardia indicated that IV Amiodarone should not be considered in these populations. KEY Point: Nothing other than AFib with WPW results in a ventricular response this fast ( which is why Figure-2 is pathognomonic for AFib in a patient with WPW ).
Or are they due to ventricular tachycardia (VT). Within about an hour, he spontaneously converted to sinus rhythm: == My Comment by K EN G RAUER, MD ( 4/23/2019 ): == Interesting rhythm — in which the tachycardia alternates from a wide to narrow QRS complex. There are no P-waves. Sinus P waves are absent.
Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered. Nevertheless, the widths of both the QRS complex and the RS duration are similar in both the old ECG and the tachycardia.
Multifocal Atrial Tachycardia 2. IJC Heart and Vasculature 25(2019). AFib is the irregularly irregular rhythm that is most commonly confused with MAT — and , AFib is much, much, much more common than true MAT. The rhythm is indeed irregularly irregular, so atrial fibrillation must be considered. GET a 12-lead!
These 5 parameters are easily remembered by the saying, “Watch your Ps, Qs & the 3 Rs” ( See My Comment in the October 16, 2019 post ). Therefore — the rhythm in ECG #1 is almost certain to be AFib ( A trial F ibrillation ) , seen here with a “rapid” ventricular response. The rhythm in Figure-1 is fast, and irregularly irregular.
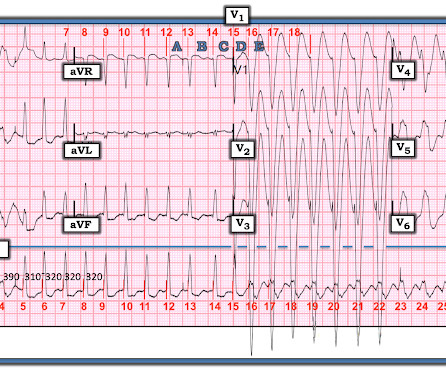
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( How would YOU interpret this tracing? How to manage the patient?
With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Am J Med 2019, 132(5):622-630. Now there is a paper published in 2019 that proves the point beyond doubt, though makes it clear that this pattern is associated with very high mortality.
ECG Blog #71 — Regarding the Ashman Phenomenon with AFib. The September 30, 2019 post in Dr. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia. Smith’s ECG Blog — for an example of “MAT”, but without the tachycardia. I link to 2 additional illustrative Cases taken from Dr. Smith’s ECG Blog.
Among the fast Supraventricular Rhythms: This is not AFib — because the rhythm is regular. The November 12, 2019 post in Dr. Smith's ECG Blog — in which I review my approach to a Regular SVT rhythm. QRS morphology that almost certainly indicates a supraventricular etiology. ECG Blog #287 — More on AFlutter.
Kazmi et al have reported on a case in which chest trauma was transiently associated with development of a Brugada-1 ECG pattern ( J Am Coll Cardiol 73 [9-Supp-1], 2019 ). Sinus Tachycardia ( common in any trauma patient. ). Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The September 22, 2019 post — intermittent ST-T wave artifact. The August 26, 2019 post — baseline artifact.
Here was his ED ECG: There is sinus tachycardia (rate about 114) with nonspecific ST-T abnormalities. An ECG was recorded: This shows a regular narrow complex tachycardia at a rate of about 160. See my quick review of atrial tachycardia below) The tachycardia spontaneously resolved. BP:143/99, Pulse 109, Temp 37.2 °C
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
49(9):808-817, 2019 ). The risk of developing TiCM depends not only on the type of tachycardia but also on the duration and the rate of the tachycardia. The "good news" is that LV function often improves, and may even return to normal IF the tachycardia can be controlled. Secondary mitral insufficiency may be seen.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content