This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. Sinus Tachycardia and RAD — as already noted above. PEARL # 2: In the absence of associated heart failure ( cardiogenic shock ) — sinus tachycardia is not a common finding in acute MI.
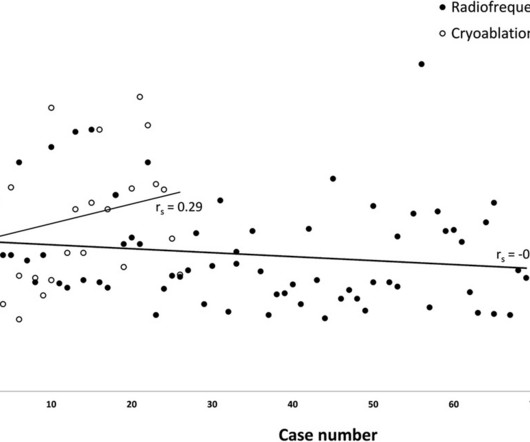
BackgroundCryoablation for pediatric atrioventricular nodal reentry tachycardia (AVNRT) is favored for reducing conduction system injury compared to radiofrequency (RF) ablation. The safety advantage of cryoablation over RF ablation primarily results from studies conducted without a three-dimensional electroanatomical mapping (3D EAM) system.
Wide-complex tachycardia: VT or aberrant, or "other?" A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Sinus tachycardia with aberrancy was unlikely as the rate was consistently 150 bpm, without spontaneous variation. And indeed the QRS morphology strongly supported VT (e.g.
There is a regular wide complex tachycardia. Remember : Adenosine is safe in Regular Wide Complex Tachycardia. Rather, from this one: Very Fast Very Wide Complex Tachycardia Ideally, one would cardiovert. An older patient with no previous medical history arrived at triage complaining of SOB. If it is VT, there will be no effect.
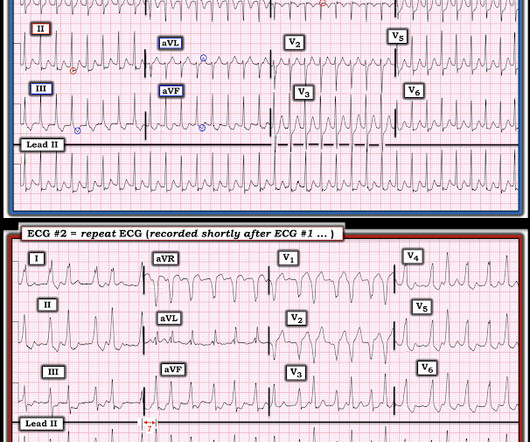
The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." Shortly after arrival, the patient spontaneously converted to this rhythm (also sent to me, along with the first): What do you think?
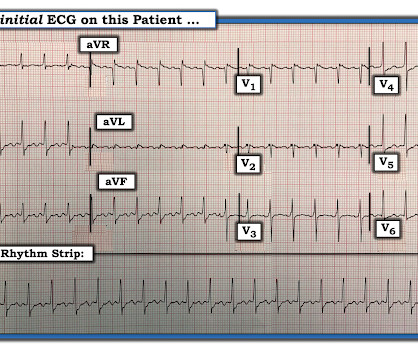
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. The Initial ECG in Today's Case: As per Dr. Meyers — the initial ECG in today's case shows sinus tachycardia with bifascicular block ( = RBBB/LAHB ). Sinus Tachycardia ( common in any trauma patient. ).
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. During tachycardia, in this case, the baseline continuously undulates especially in leads II, aVR and V1; very good for atrial flutter.
This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ).
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Comment by K EN G RAUER, MD ( 12/11/2018 ): = I love this case — because it brings home 3 of my favorite teaching points about electrolyte disorders and ECG interpretation. It is safe even when there is no hypocalcemia, but is particularly safe if there is hypocalcemia, which you can infer from a long ST segment.
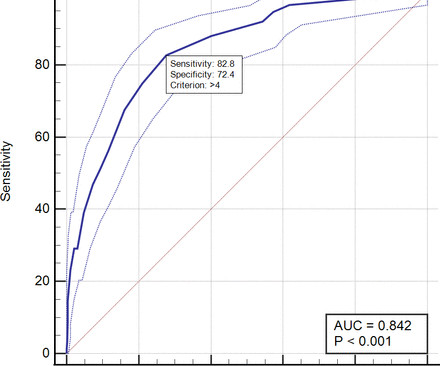
Methods This retrospective cohort study included all ACS patients aged≥18 years who were admitted to Dr. Hasan Sadikin Central General Hospital from January 2018 to January 2022. The area under the curve (AUC) among PADMA, GRACE, C-ACS and ProACS risk scores was compared using the fisher Z test.
Tachycardia and ST Elevation. == MY Comment , by K EN G RAUER, MD ( 7/7 /2024 ): == Among the most rewarding type of case for me during my days working in the ED — would be seeing a patient who presented with acute CP ( C hest P ain ) — who I would be able to “cure” simply by recognizing and treating their arrhythmia. Would you give lytics?
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think?
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
Since partnering with Vector Remote Care in 2018 , Wellstar has succeeded in triaging urgent alerts more quickly, reducing time to treatment, and decreasing hospitalizations. Thanks to SmartReports’ prioritization of the alert, Heather and her team contacted the patient and scheduled an immediate appointment within 15 minutes.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
Tachycardia (or nearly) 2. Tachycardia, = 1.8. Finally , they found these independent predictors of PE: Note that tachycardia only has an Odds ratio of 1.8. Tachycardia is unusual in ACS unless there is cardiogenic shock or a second simultaneous pathology. Some providers were worried about ACS because of this ECG.
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Tachycardia and ST Elevation. Christmas Eve Special Gift!! Is this inferor STEMI?
Here was the ECG: There is sinus tachycardia. This was sent by a reader. A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. and K was normal. This is "Shark Fin" morphology. Smith — this case was not what I thought. I did recognize the S hark F in m orphology of dramatic ST elevation.
The principal d ifferential d iagnosis i s similar to what we derived in the October 16, 2019 Case : i ) Sinus Tachycardia ; ii ) Reentry SVT ( either A VNRT if the reentry circuit is contained within the normal AV nodal pathway — or A VRT if an accessory pathway is involved ) ; iii ) Atrial Tachycardia ; or iv ) Atrial Flutter.
The ECG there reportedly showed an irregular tachycardia, and the patient was immediately referred to the emergency room. Here is her ECG on arrival: There is a wide complex tachycardia that is irregularly irregular (this is difficult to determine at these very high rates). Vitals were within normal limits other than heart rate.
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ).
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
Can J of Cardiol 2018, 34: 132-145 Here are some other cases: LVH, LBBB, RBBB, and RVH may manifest ST depression without any ischemia! Methods STEMI activations between January 2014 and April 2018 at the University of Arizona Medical Center were identified. Miranda DF, Lobo AS, Walsh B, et al. A normal PR interval.
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. Because the SA node is sick the SA node recovery time is often prolonged, which is why long pauses most commonly follow episodes of tachycardia ( which produced SA node suppression ).
2 short runs of SVT ( presumably atrial tachycardia ). 2 short runs of SVT ( presumably atrial tachycardia ). The July 5, 2018 post in Dr. Smith's ECG Blog — ( Please see My Comment at the bottom of the page for Review on the ECG diagnosis of S ick S inus Syndrome). Bradycardia was not limited to nighttime hours.
This is sinus tachycardia at a Rate of ~115/minute. For more on the ECG findings when leads V1 and V2 are placed too high on the chest — Please SEE My Comment at the bottom of the page in the November 4, 2018 post of Dr. Smith’s ECG Blog ). The Rhythm is regular and rapid. Simply repeat the ECG after verifying correct lead placement.
Sinus Tachycardia ( common in any trauma patient. ). 72; Issue 9; 2018 ) — A ) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. — Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ).
A b rief chart review revealed his most recent echo in 2018, with LV EF 67%, “very small” inferior wall motion abnormality. I find AV dissociation in VT to be very difficult to differentiate from artifact, as there are always random blips on tachycardia tracings. Past medical history includes coronary stenting 17 years prior.
We have often referred to this almost magical m irror- i mage r elationship for ST-T waves in leads I II and aV L — which when present, means a cute i nferior O MI until you prove otherwise ( See My Comment on the 8/9/2018 SSmith Blog Post ). CLICK HERE — for my detailed discussion of this subject ).
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
Ventrax is intended to facilitate placement of devices used in ablation procedures commonly performed to treat an abnormally fast heartbeat known as ventricular tachycardia (VT). Retrograde Aortic Access During Ventricular Tachycardia Ablation: Indications, Techniques, and Challenges. commercial release of its Ventrax Delivery System.
The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact. The January 30, 2018 post — for PTA. The rhythm terminated before it could be captured on 12-lead.
2) Tachycardia to this degree can cause ST segment changes in several ways. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia. Is this inferor STEMI? Atrial Flutter with Inferior STEMI? What is the Diagnosis?
Introduction:Supraventricular tachycardia (SVT) is common and poorly tolerated in patients who have undergone Fontan procedure. Rate of recurrence did not differ between those who had the procedure before or after 2018. Atrial Tachycardia (70%) and Typical Atrial Flutter (65%) were the most common SVTs ablated.
There is a regular, wide complex, (mostly) monomorphic tachycardia. The differential of wide, regular, monomorphic tachycardia is: VT or SVT with aberrancy, all +/- hyperkalemia (see diagrams below). Really wide tachycardia = VT or SVT with conduction abnormality + hyperkalemia, until proven otherwise.
Chagas disease (ChD) was associated with increased rates of ventricular tachycardia and ventricular fibrillation in ICD patients only in the initial two periods, but there was no statistical difference in the last period. Methods This retrospective observational study included patients who received ICDs between October 2007 and December 2018.
NOTE: For those wanting more practice recognizing Shark Fin ST-T wave changes — we've shown cases of this entity in the following ECG Blog posts ( among others ): In the June 11, 2018 post — In the October 4, 2019 post — In the November 22, 2019 post — in the January, 24, 2020 post — in the February 16, 2020 post — in the April 25, 2020 post — in the (..)
This study aimed to create a preprocedural screening tool to identify patients at risk of non-PV triggers during first-time AF ablation.METHODS:All patients who underwent first-time AF ablation at the Hospital of the University of Pennsylvania between 2018 and 2022 were identified.
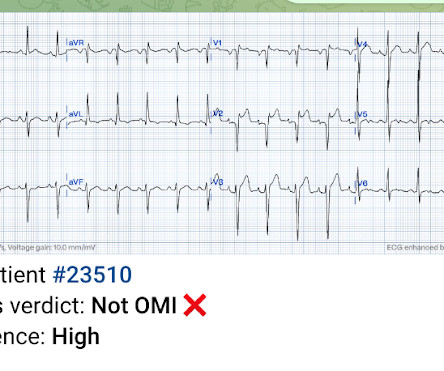
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content