This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
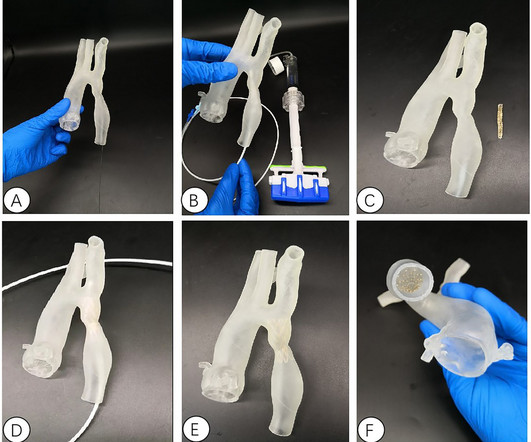
and an investigator in the VIVID study , which contributed to the device’s FDA approval – successfully used the Duo Venous Stent System for the first time outside of a clinical trial. Duo Hybrid has a distinct integrated design that combines multiple zones of differing mechanical properties into a single stent [3].
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
M2‐M4, ACA, and PCA) who underwent thrombectomy over 5 years (2018‐2022) at a single comprehensive stroke center. M2‐M4, ACA, and PCA) who underwent thrombectomy over 5 years (2018‐2022) at a single comprehensive stroke center. Primary safety outcome is rate of complications associated with the stent retriever.
The clinical data during hospitalization and follow-up were analyzed.ResultsAll the patients of CoA were successfully treated with percutaneous balloon dilatation covered stent implantation. There were 6 males and 4 females whose average age was (27.6813.45) years. The narrowest average diameter of CoA increased from (4.352.61)mm
Diseased human arteries are most simply, reliably, and successfully treated with drug-eluting, balloon-expandable stents," said Lewis B. Encouraged by the early clinical results, Efemoral Medical is now developing an additional device for treating below-the-knee (infrapopliteal) arteries in patients with CLTI. Eur J Vasc Endovasc Surg.
Doctors then treat the cause of the heart attack, either inserting a stent, removing a clot or taking other necessary action. approximately 80,000 people are diagnosed with cardiogenic shock as a result from a heart attack each year according to data from a published study that looked at a 15-year trend from 2004 to 2018. In the U.S.,
If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Since the FFR wire can be used for guiding balloon catheters and stents, it is easy to make post procedure measurements without any additional effort. Routine FFR measurement probably lead to more judicious use of stents and improved outcomes.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
Method Between June 2018 and December 2022, 62 patients with type A aortic dissection (TAAD) underwent reoperation after previous surgical treatment. Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period.
In-stent restenosis was excluded. In the DCB group, 43 patients (29.2%) were treated with DCB only and 104 (70.8%) with a hybrid approach; DCB length was greater than stent length in 55.1% The DCB group included both patients undergoing DCB-only PCI and those receiving hybrid PCI with DCB and DES combined. versus 83.5%;P=0.036)
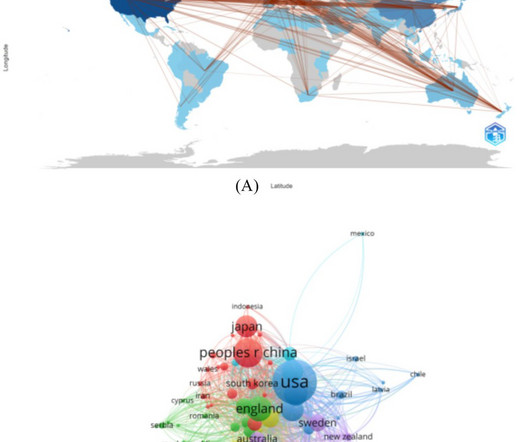
The most cocited reference was Chaikof EL, 2018, J Vasc Surg, v67, p. Artificial intelligence, clinical outcomes and bridging stent were the primary keywords of emerging research hotspots.ConclusionThis is the first bibliometric study to comprehensively summarize the research trends in abdominal aortic aneurysm research.
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. Here is the PMcardio version: Because the Queen diagnosed OMI with High Confidence, the cath lab was activated without bothering a physician. Then the high sensitivity troponin T returned at 1400 ng/L.
Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. In this view, the culprit lesion is not particularly obvious which is an important principle in angiography, and the reason why we obtain multiple views.
Past medical history includes coronary stenting 17 years prior. A b rief chart review revealed his most recent echo in 2018, with LV EF 67%, “very small” inferior wall motion abnormality. Pretest probability: Even before the ECG, a patient with a history of coronary stent has a 90% chance that his wide complex tachycardia is VT.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. The patient was transferred to CCU to consider surgical options.
ml/h, P = 0.04), a higher likelihood of parent artery stenosis (65% vs. 20.8%, P < 0.001), and increased need for angioplasty or stenting (50% vs. 17%, P < 0.001). Follow-up lesion volumes and functional outcomes were similar; however, the mismatch group showed a slower infarct growth rate (3.8 ml/h vs. 7.5 vs. 21.2%, P = 0.02).Conclusions:DWI-ADC
Intravascular imaging (IVI), such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), play a crucial role in assessing lesion characteristics and optimizing stent placement during percutaneous coronary intervention (PCI). Patients were divided into two groups based on IVI usage.
At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. As I illustrated in detail in My Comment of the October 3, 2018 post of Dr. Smith's ECG Blog — I favor a qualitative approach based on shape.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe Coil embolization was performed for fifty‐four patients using various adjunctive techniques (simple, 7; double catheter, 15; balloon neck remodeling, 7; stent‐assisted, 26 (LVIS Jr.,
Here we assess the efficacy of technique switching after the first pass failed reperfusion in a large multi-center cohort.Methods:All consecutive patients treated with EVT from 12 centers across the US were prospectively collected between 10/2018 12/2021 (SVIN Registry). Exclusion criteria included incomplete data.
Optimal management is controversial, with options including medical therapy (MT), endovascular stenting (ES), and surgical revascularization (SR). Propensity scores adjusted for baseline differences.
The purpose of this study was to compare the outcomes of EVT for ICAD with those of cardiogenic cerebral embolism (CE) based on real-world data from a multicenter, prospective registry study (K-NET registry) involving 40 centers in Japan.Methods:The K-NET study enrolled 3187 EVTs in 2018-2021, of which 358 (11%) were ICAD and 1870 (59%) were CE.
We aimed to evaluate the association between RS with functional outcomes compared to medical management (MM) in patients who underwent failed MT.Methods:This is a cross-sectional study using prospectively collected data from the Society of Vascular and Interventional Neurology (SVIN) Registry from 2018 to 2021.
Background:Postoperative complication rates of carotid endarterectomy (CEA) and carotid artery stenting (CAS) for carotid artery stenosis are recommended to be maintained below a certain threshold. Stroke, Volume 56, Issue Suppl_1 , Page ATP128-ATP128, February 1, 2025.
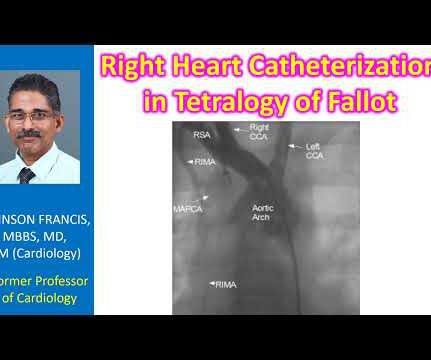
Stenting of the patent ductus arteriosus can be considered in neonatal period for improving oxygen saturation till corrective surgery. 2018 Jun 28;3:e72-e79. Anomalous coronary arteries can cross the right ventricular outflow tract and can be damaged during procedures needed for widening of the RVOT. References Wagdy R. 2018.76824.
In 2018, he even opened a state of the art lab nicknamed “the Watcher” and was paid $18 million from Medicare in the next 3 years. Dormu, who on the same day, performs another angiogram which revealed an in-stent restenosis of the superficial femoral artery stent and a 60% stenosis of the tibioperoneal trunk.
Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ). The February 11, 2020 post ( LA-RA reversal ).
One would not expect wall motion to recover so quickly after stenting, so this is good evidence that the POCUS echo was indeed accurate. Angiogram: Severe diffuse left main disease, up to 80% at the ostial left main. Post cath ECG: Normal or near normal Peak troponin I was 15 ng/mL.
The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. Patient 2 Clinical Course and Outcome: This patients first ECG was sent to the EM physician who said it did not meet STEMI criteria, but wisely agreed with EMS to get serial ECGs during transport. The cath lab was now activated.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
He did, found the true culprit, and went back in to stent it. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. Right Ventricular MI seen on ECG helps Angiographer to find Culprit Lesion This is the ECG.
One stent was deployed with restorative TIMI-0 flow. However, when the Troponin I returned 8.4 ng/mL during the night – in the presence of unmitigated pain – cardiology decided to take him to the Cath Lab. The red arrow shows a 90% LAD occlusion at the D1 branch. it has been subsequently deemed a STEMI-equivalent.
He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. This is to suggest improved TIMI flow – most likely a combination of the ASA administration in tandem with the body’s own natural tPA – yet the ECG still retains signatures of an active thrombus. 3] Aslanger, E.,
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. A 99% LAD occlusion was stented. BP 110/67 HR 68 RR 14 (non-labored) SpO2 95 RA Physical exam revealed slight pallor and diaphoresis. Attached is the first ECG. 5] Walsh, B.
The total occlusion was recanalized and stented from 100 to 0%. ii ) Since it is now 7 years since initial publication of the OMI Manifesto ( See the April 18, 2018 post in Dr. Smith's ECG Blog ) We would have expected that emergency providers ( especially cardiologists!
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6. Progression of V2 showing posterior involvement.
Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented. The nearest PCI center was activated but ultimately denied by Cardiology. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergency department patients. 2] Costanzo, L.
They found an acute lesion of the LAD at the site of the prior stents, including 70% proximal LAD lesion and 95% mid-LAD stenosis with TIMI 3 flow at the time of cath. The LAD lesion was acute and required 3 stents to restore flow. They took him almost immediately for catheterization.
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 2018 Sep 6;379(10):924-933. But that’s a whole can of worms for another day). Medicine (Baltimore).
It was stented. My Comment , by K EN G RAUER, MD ( 10/24/2018 ): = Important teaching points are made in this post by Dr. Smith. We have previously discussed this phenomenon ( Please see the P.S. at the bottom of the page in My Comment, from Dr. Smith’s July 11, 2018 blog post ). Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5,
A mid-LAD culprit lesion was identified and stented. Cardiology felt her chest pain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution. Pacing Clin Electrophysiol. 40; 1234-1241.
Angiogram showed a distal RCA occlusion which was stented. While the cath lab was getting ready, we recorded a right sided ECG: V1=V1R which is the same location as V2 V2 = V2R = same location as V1 V3-V6 = V3R - V6R Inferior MI is obvious There is no right ventricular MI evident on these ECGs. Echo showed inferior wall motion abnormality.
Ed Burns has a very nice complete summary of Wellens' syndrome here: [link] = Comment by KEN GRAUER, MD ( 6/28/2018 ): = Highly insightful post with superb explanation by Dr. Smith, illustrating by sequential evolution over 5 serial tracings what Wellens’ Syndrome is, and what it is not. Here is the first post-cath ECG (ECG #4).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content