This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. A near 60 year old male called 911 for increasingly severe fever and SOB.
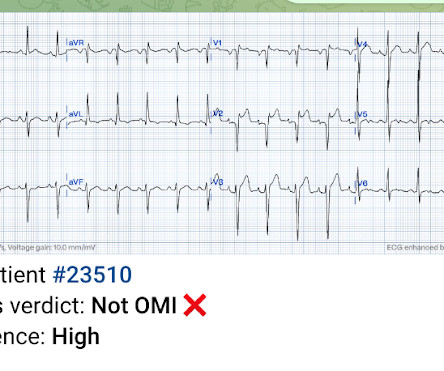
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia. What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
Here was the ECG: There is sinus tachycardia. So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? This was sent by a reader. A previously healthy 53 yo woman was transferred to a receiving hospital in cardiogenic shock. and K was normal. Which artery?
There is sinus tachycardia. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology. I have always said that tachycardia should argue against acute MI unless there is cardiogenic shock or 2 simultaneous pathologies. Here is that ECG: What do you think?
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrial flutter. Is this inferor STEMI? Tachycardia and ST Elevation. Christmas Eve Special Gift!!
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. A very small QRS complex can only mount a very small amount of STE. This patient had a full RCA occlusion with the smallest visible STE. Baseline and serial ECGs make you much more likely to identify OMI.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. 2) Tachycardia to this degree can cause ST segment changes in several ways. Is that an obvious STEMI underneath that rhythm? If I fix the rhythm will the ST changes resolve?
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. Did YOU Notice that the underlying rhythm in Figure-1 appears to be atrial tachycardia?
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". After initiating treatment for hyperkalemia, repeat ECG showed resolution of Brugada pattern: The ECG shows sinus tachycardia. A Very Wide Complex Tachycardia. From Ken Grauer ( See below ) — with this Figure adapted from LITFL.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. 2] But there is also Sinus Tachycardia! Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Closer inspection will show that it is Sinus, after all.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. A rectal temperature was obtained which read 107.9 Bicarb 20, Lactate 4.2,
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. STEMI was activated and the patient went to Cath on arrival. There may even be significant overlap between these factors. link] [1] Mirand, D. 2] Aslanger, E.,
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Heart Rhythm 2018. Her temperature was 106 degrees. Hyperkalemia 2.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. Taken together, these findings suggest an ongoing extensive antero-lateral STEMI. I don't know what the device algorithm interpretation stated. The final angiographic result is very good.
Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. If the QRS is prolonged, then the differential includes: 1. Hyperkalemia 2. Other drugs with sodium channel blockade: Tricyclic antidepressants.
Whereas the patient's initial ECG shows sinus rhythm and nonspecific ST-T wave abnormalities just 24 minutes later , there is now profound bradycardia with a junctional escape rhythm ( YELLOW arrows highlighting retrograde P waves ) and obvious findings of an acute inferior STEMI. Circulation Research , 114 (12), 18521866. Kontogiannis, C.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content