This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardial infarction (STEMI).MethodsA
European Heart Journal , ehy651, [link] Published: 26 October 2018 [link] Timing of revascularization in patients with transient ST-segment elevation myocardial infarction: a randomized clinical trial. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded.
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
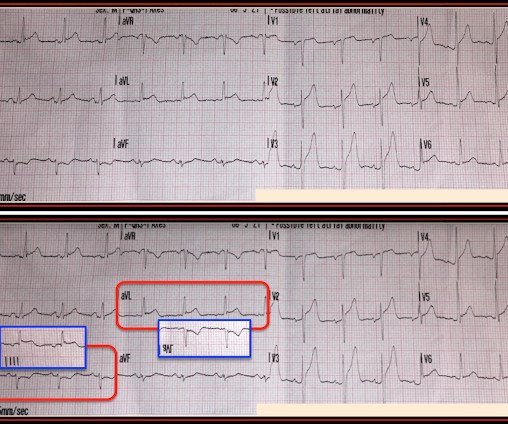
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The July 31, 2018 post in Dr. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ).
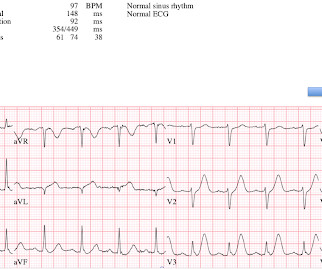
IMPRESSION: In this patient who presents with severe, new-onset CP — today's ECG is diagnostic of an extensive, ongoing antero-lateral STEMI. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Saddleback ST Elevation is almost never STEMI 2. An inverted P-wave in lead V2 implies lead misplacement too high Saddleback in STEMI: Here are the only 2 ECGs with V2 "saddleback" that I have ever seen which really represented an LAD Occlusion: Anatomy of a Missed LAD Occlusion (classified as a NonSTEMI) A Very Subtle LAD Occlusion.T-wave
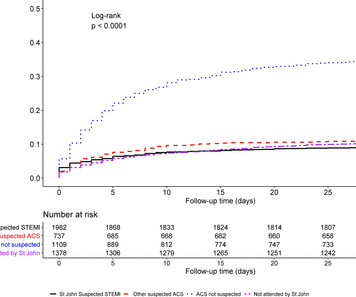
Background Early recognition of ST-segment elevation myocardial infarction (STEMI) is needed for timely cardiac monitoring and reperfusion therapy. Results Of 5465 patients with STEMI, 73% were transported to hospital by ambulance. and non-ACS diagnosis in 29.7%.
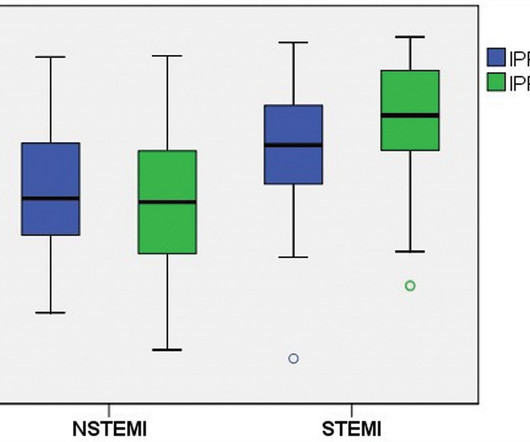
Methods Clinical data from patients admitted to the cardiology division between 2018 and 2022, who were diagnosed with AMI and underwent an IPF testing. Results Among the 277 patients diagnosed with AMI who underwent IPF testing, 113 had (STEMI) and 164 had (NSTEMI). Notably, among STEMI patients, those with IPF ≥ 4.2%
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
October 2018. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. Fair enough.
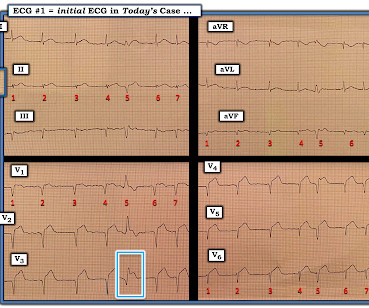
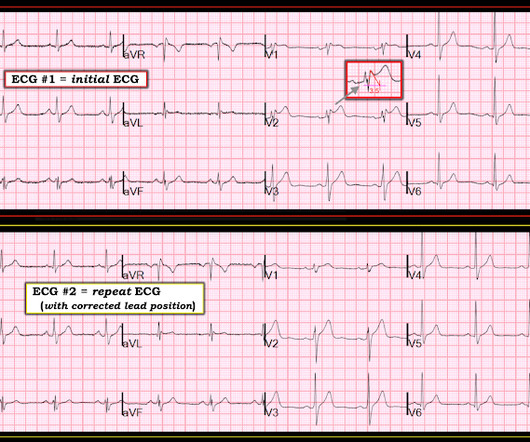
P utting I t A ll T ogether : After correcting for LA-LL lead reversal — ECG # 1a shows sinus rhythm — LVH — and an acute infero-postero STEMI with acute RV involvement. PEARL # 3: In the absence of an anterior STEMI — acute inferior MI is the result of either acute RCA or LCx ( L eft C ircumfle x ) coronary occlusion.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. My Comment , by K EN G RAUER, MD ( 10/24/2018 ): = Important teaching points are made in this post by Dr. Smith. A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 1 1/2 hours.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ).
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 In the 500+ Comments I have written on Dr. Smith's ECG Blog since becoming an Associate Editor in 2018 — I do not believe we have had a case of RA-LL lead reversal. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ).
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
[link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….) it has been subsequently deemed a STEMI-equivalent.
The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. Then the high sensitivity troponin T returned at 1400 ng/L.
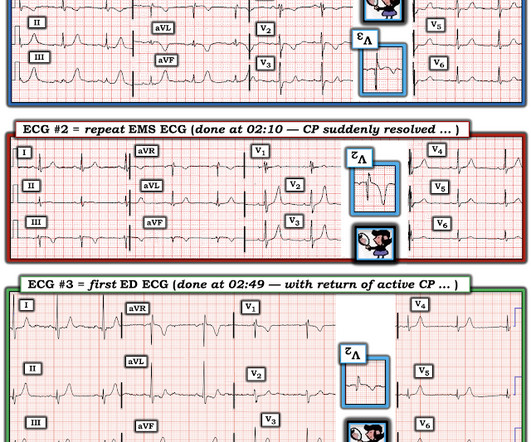
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. KEY Point: The best way to confirm acute RV MI — is with use of right -sided leads ( See My Comment in the July 19, 2020 and July 11, 2018 posts). During EMS transport, the pain suddenly resolved.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. 2 prior ECGs were found in his medical record — the latest of which was done circa 2018 ( which would be ~8 years after his inferior MI — and ~5 years before ECG #1 ).
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Eur Heart J 2018. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. This is a "Transient OMI".
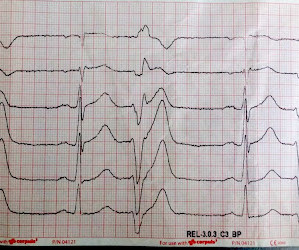
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? It is often confused with a wide QRS due to conditions such as hyperkalemia. Which artery? There is ST Elevation in every lead except aVR (STD in aVR). Could this be myopericarditis?
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I Steffen wrote: " I remembered the ECG from your blog titled: "STEMI Seen Best in PVC, Diagnosed by Medic, Ignored by Physician" from 2013. I also put them side by side: What do you think?
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria. The STEMI vs. NSTEMI paradigm is not the best way to decide who needs emergent reperfusion therapy.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. For more on this topic — See discussion in the October 24, 2019 and July 31, 2018 posts in Dr. Smith's ECG Blog ).
If it is STEMI, it would have to be RBBB with STEMI. Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018 ). == Distinction is made between 2 types of Brugada ECG patterns: A B rugada - 1 ECG pattern — shows ≥2 mm coved ST elevation with sharp downslope plus T wave inversion in ≥2 anterior leads.
Another overlooked OMI ( Cardiologist limited by STEMI Definition — OMI evident by Mirror Test ) — See My Comment at the bottom of the page in the September 21, 2020 post on Dr. Smith’s ECG Blog. Smith’s ECG Blog.
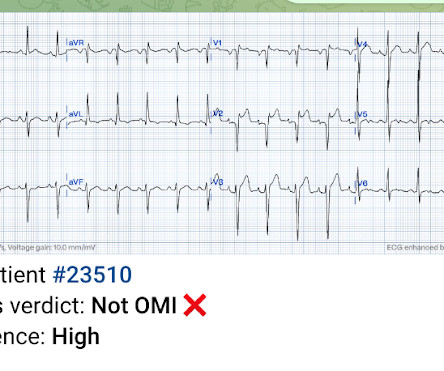
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria. Meyers, Weingart and Smith in their 2018 OMI Manifesto.
It tells us there is an active, ongoing process — and that prompt cath with acute reperfusion is likely to be needed regardless of whether or not the millimeter-definition of a STEMI has been satisfied. The July 31, 2018 post in Dr. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ).
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. 72; Issue 9; 2018 ) — A ) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. —
Here is our abstract from SAEM 2018. The MSC were highly sensitive and specific for the diagnosis of ACO in patients presenting to the ED with VPR and symptoms of acute coronary syndrome. == MY Comment , by K EN G RAUER, MD ( 10/3 /2018 ): == How good are paced tracings for detecting ACO ( A cute C oronary O cclusion ) ?
Here is a repeat ECG 45 minutes later with persistent chest pain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3. Repeat ECGs make difficult decisions easier. -- Comment by K EN G RAUER, MD ( 12/29/2018 ): -- Superb case by Dr. Pendell Meyers, which highlights recognition of subtle acute findings.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content