This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
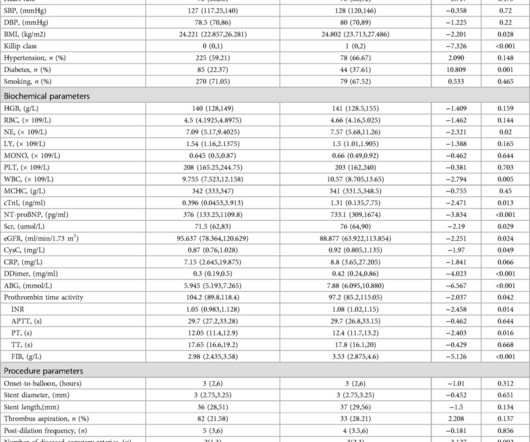
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardialinfarction (STEMI).MethodsA
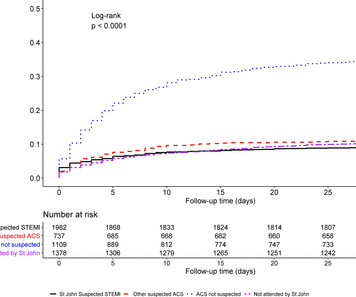
Background Early recognition of ST-segment elevation myocardialinfarction (STEMI) is needed for timely cardiac monitoring and reperfusion therapy. Results Of 5465 patients with STEMI, 73% were transported to hospital by ambulance. and non-ACS diagnosis in 29.7%.
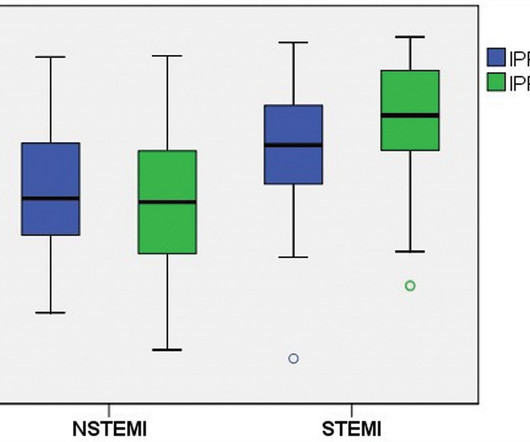
Introduction Elevated peak cardiac troponin levels have been linked with increased morbidity and mortality in patients with acute myocardialinfarction (AMI). Methods Clinical data from patients admitted to the cardiology division between 2018 and 2022, who were diagnosed with AMI and underwent an IPF testing.
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
European Heart Journal , ehy651, [link] Published: 26 October 2018 [link] Timing of revascularization in patients with transient ST-segment elevation myocardialinfarction: a randomized clinical trial. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial.
There is an obvious inferior posterior STEMI(+) OMI. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. What is the atrial activity? Is it sinus arrest with junctional escape?
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. No further troponins were drawn. Why is this important?
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. October 2018. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. Am J Emerg Med 36(10):1771-1774.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
If it is STEMI, it would have to be RBBB with STEMI. Only 5-18% of ED patients with chest pain have a myocardialinfarction of any kind. The patient presented with chest pain. Here is the ECG: What do you think? I frankly did not know what to think. Is it Brugada pattern? But in a very unusual pattern. Only 1-5% have OMI.
Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Impact of total occlusion of culprit artery in acute non-ST elevation myocardialinfarction: a systematic review and meta-analys is.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? Am Heart J.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. But which myocardial walls are affected? Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. Unusual and puzzling, as there was a large focal acute MI) Final Diagnosis: Acute MI, Non ST Elevation MyocardialInfarction.
This is a troponin I level that is almost exclusively seen in STEMI. In this case, profound shock for 1 hour would result in the same degree of infarction. A followup ECG was recorded 2 days later: No definite evidence of infarction. So this is either a case of MINOCA, or a case of Type II STEMI. Troponin I rose to 44.1
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria.
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. STEMI was activated and the patient went to Cath on arrival. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute MyocardialInfarction in the emergency department. link] [1] Mirand, D.
Smith, MD – Department of Emergency Medicine, Hennepin County Medical Center, Professor, University of Minnesota School of Medicine, Minneapolis, MN ABSTRACT: Background: Patients with type 1 myocardialinfarction with normal left ventricular function that are hemodynamically stable do not usually manifest with sinus tachycardia.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chest pain from an 8/10 to 4/10. NTG drip started. Pain better still. Is this OMI?
It is equivalent to a transient STEMI. This is diagnostic of myocardialinfarction. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department.
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. Is that an obvious STEMI underneath that rhythm? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? If I fix the rhythm will the ST changes resolve?
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. As the conversation progressed, another ECG spontaneously printed. 2] Driver, B.
Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) A recent study found that SCAD causes almost 20% of STEMI in young women. examined SCAD presenting as STEMI (unlike Hassan et al. A study by Hassan et al. Lobo et al. where more than 3/4 of cases were NSTEMI).
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Am J Cardiol 2018; 122(8):1303-1309. Annals of Emergency Medicine 2012;60:45-56. QTc is the computer measurement.
Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction. Occlusion MyocardialInfarction (OMI) often does not present with diagnostic ST elevation, or even any STE, especially in dialysis patients.
Relying on troponin elevation to diagnose acute coronary occlusion after at least 4 hours of infarction when the ECG can identify it immediately is poor choice. 3) STEMI criteria failed to identify this acute coronary occlusion, like many others. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardialinfarction patients. How does the Queen of Hearts do? Ann Emerg Med [Internet]. 2012;60:766–776. 2023;131569.
BACKGROUND:Sex differences in acute myocardialinfarction treatment and outcomes are well documented, but it is unclear whether differences are consistent across countries. 1 in 2018; Israel NSTEMI ratio, 1.71:1 1 in 2018). 1 in 2018; Israel NSTEMI ratio, 1.71:1 1 in 2018). 1 in 2011 and 1.73:1
Smith: T waves are very hyperacute: these are a sign of ACUTE infarction, even if there are Q-waves. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). See Raitt et al.:
The authors describe a case with some features in common with our patient -- a stressful event followed by a stress cardiomyopathy/acute myocardialinfarction overlap syndrome. Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. Acute myocardialinfarction triggered by emotional stress.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. The January 30, 2018 post — for PTA. There are new Q-waves in aVL, V5-6.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content