This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
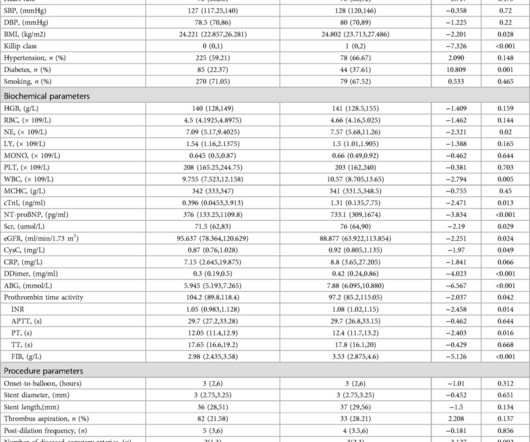
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardialinfarction (STEMI).MethodsA
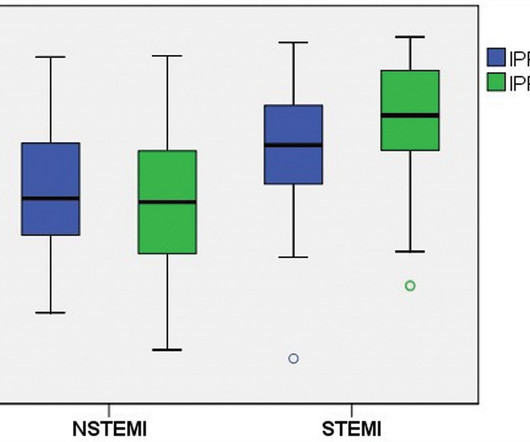
Introduction Elevated peak cardiac troponin levels have been linked with increased morbidity and mortality in patients with acute myocardialinfarction (AMI). We hypothesize that patients with higher IPF levels during AMI, will experience a more severe infarct, leading to elevated peak troponin levels.
Background:Type 2 myocardialinfarction (T2MI) and type 1 myocardialinfarction (T1MI) differ with respect to demographics, comorbidities, treatments, and clinical outcomes. This could facilitate more accurate longitudinal assessments of acute myocardialinfarction quality and outcomes. T1MI and 53.5%
BackgroundValsartan was recalled by the US Food and Drug Administration in July 2018 for carcinogenic impurities, resulting in a drug shortage and management challenges for valsartan users. Journal of the American Heart Association, Ahead of Print. The influence of the valsartan recall on clinical outcomes is unknown.
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardialinfarction (STEMI).
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. Eur Heart J 2018. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty.
Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). Immediate and early percutaneous coronary intervention in very high‐risk and high‐risk non‐st segment elevation myocardialinfarction patients.
Safety was defined by MACE (major adverse cardiac events) inclusive of type 1 myocardialinfarction (MI) in patients discharged from ED, and clinical effectiveness by percentage ED discharge. of the cohort) with no safety signal (MACE rate 4/444 (0.9%) vs 4/769 (0.52%), p=0.430 for the 2011 and 2018 cohort, respectively).
Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). 2009;54:386–393.
In the present study, we compared the outcomes and cost of a VCR versus traditional CBCR program.Methods and ResultsIn a retrospective cohort study comparing VCR versus CBCR, CBCR data were collected from a period of January 2018 to September 2023. VCR data were collected from program initiation in July 2021 to September 2023.
Self-reported smoking status was assessed at each consecutive visit and used to determine smoking cessation after each interim ASCVD event (myocardialinfarction, percutaneous coronary intervention, coronary artery bypass graft, stroke/transient ischemic attack, peripheral artery disease).
Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. International evaluation of an artificial-intelligence- powered electrocardiogram model detecting acute coronary occlusion myocardialinfarction. Clin Cardiol 2022 4.
This study evaluated the relationship between community-level distress and CR participation, access to CR facilities, and clinical outcomes.METHODS:A retrospective cohort study was conducted on a 100% sample of Medicare beneficiaries undergoing inpatient coronary revascularization between July 2016 and December 2018.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
This typically occurs after an inferior posterior myocardialinfarction, drug-induced CHB. 2018 Jun;52(1):111-116. Epub 2018 Mar 12. Here is a patient, where a permanent pacemaker was kept temporarily for a few weeks or a month in high-risk reversible complete heart block situations. J Interv Card Electrophysiol.
Methods We analyzed a cohort of patients admitted for ACS between February 2017 and February 2018. Aim The aim of this study was to determine the best clinical predictors of acute heart failure needing mechanical ventilation (MV) in the first 48 h of evolution of patients admitted because of acute coronary syndrome (ACS).
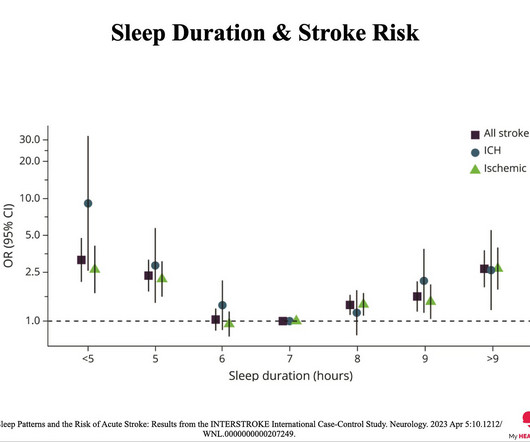
2018 Apr 10;90(15):e1298-e1305. 5 Sleep Duration and MyocardialInfarction. If you want to know more about a consultation with Dr Barrett, Click Here or on the button below. I'm Interested In Case You Missed Them: 1 Midlife cardiovascular fitness and dementia: A 44-year longitudinal population study in women. JAMA Intern Med.
Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardialinfarction. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardialinfarction (DIFOCCULT study). Eur Heart J 2018 4. Int J Cardiol Heart Vasc 2021 2. Aslanger et al.
(Unusual and puzzling, as there was a large focal acute MI) Final Diagnosis: Acute MI, Non ST Elevation MyocardialInfarction. The presence or absence of ST Elevation is a poor marker with which to describe a myocardialinfarction. = NSTEMI is extremely heterogenous, from a very tiny Non-OMI to a massive OMI.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. As I illustrated in detail in My Comment of the October 3, 2018 post of Dr. Smith's ECG Blog — I favor a qualitative approach based on shape.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
Smith, MD – Department of Emergency Medicine, Hennepin County Medical Center, Professor, University of Minnesota School of Medicine, Minneapolis, MN ABSTRACT: Background: Patients with type 1 myocardialinfarction with normal left ventricular function that are hemodynamically stable do not usually manifest with sinus tachycardia.
This is obviously diagnostic of inferior and lateral Occlusion MyocardialInfarction. The location of the infarct is clear, but that does not necessarily tell you what artery it is. Electrocardiographic diagnosis of acute coronary Occlusion MyocardialInfarction in ventricular paced rhythm using the modified Sgarbossa criteria.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. The “bottom line” conclusions of their case report were that transient J waves may on occasion be induced by an acute injury current from impending myocardialinfarction.
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardialinfarction, likely proximal LAD or Left main." EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chest pain from an 8/10 to 4/10. NTG drip started. Pain better still.
This is diagnostic of myocardialinfarction. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. She felt more comfortable being admitted. Int J Cardiol.
MINOCA: MyocardialInfarction in the Absence of Obstructive Coronary Artery Disease). Shark Fin morphology has been discussed a number of times on Dr. Smith’s ECG Blog ( For review — See the June 11, 2018 post and the January 24, 2020 post , to name just 2 instances ). I believe the latter (type II STEMI) is most likely.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Can J of Cardiol 2018, 34: 132-145 Here are some other cases: LVH, LBBB, RBBB, and RVH may manifest ST depression without any ischemia! Am J Med 2019, 132(5):622-630. link] Harhash AA et al.
He was found diaphoretic and uncomfortable, and verbalizing a prior history of myocardialinfarction and that, furthermore, the acute symptoms were identical to that which had been associated with RCA stent placement 4 years prior. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization.
Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardialinfarction. With deliberate practice, spot diagnosis of T-to-R ratio will come with time. References 1] Smith, S. Annals of Emergency Medicine, 60 (1), 45-56. 2] Driver, B. Journal of Electrocardiology, 50 , 561-569.
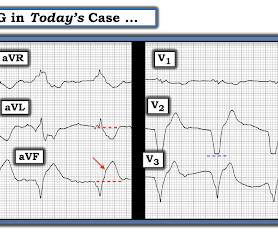
Here it is: Computer Interpretation: SINUS RHYTHM INFERIOR MYOCARDIALINFARCTION, POSSIBLY ACUTE ST ELEVATION, CONSIDER ANTERIOR INJURY [MARKED ST ELEVATION W/O NORMALLY INFLECTED T WAVE IN V2-V5] ACUTE MI What do you think? This ECG was texted to me with no information: I answered: "Show me the whole 12-lead."
Many of these issues were described in a prior post by Dr. Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.) Revascularization in Patients With Spontaneous Coronary Artery Dissection and ST-Segment Elevation MyocardialInfarction. References Lobo AS et al.
New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Paroxysmal atrioventricular block: Eletrophysiological mechanism of phase 4 conduction block in the His-Purkinje system: A comparison with phase 3 block. Pacing Clin Electrophysiol. 40; 1234-1241.
ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. This confirms that there were dynamic signs of ischemia on the initial ECG. It was not normal! A third troponin I returned at 0.27 Epilogue : Angiography, however, did not reveal significant obstruction of the RCA, LAD, or circumflex.
Diagnostic and prognostic value of the QRS-T-angle, an ECG marker quantifying heterogeneity of depolarization and repolarization, in patients with suspected non-ST-elevation myocardial infarc tion. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6.
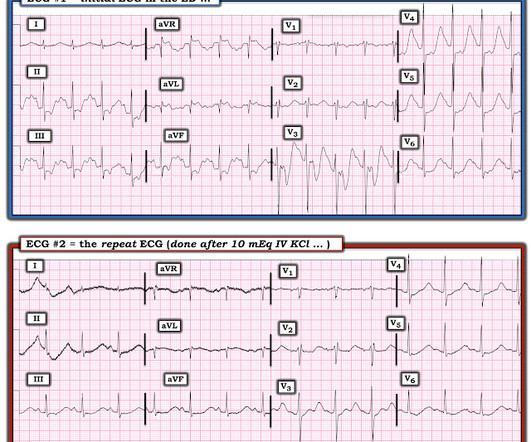
This was not a myocardialinfarction of any kind. Possible inferior and infero-lateral WMA are new The next AM, the K had come up to 2.3 mEq/L: It is normalizing Troponins reached a peak of 42 ng/L (URL = 34 ng/L). Learning Points: 1. When the EKG looks bizarre, think about pulse tapping artifact 2.
Diagnosis of acute myocardialinfarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads. Acute myocardialinfarction due to left circumflex artery occlusion and significance of ST-segment elevation. From AM et al.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. Am J Cardiol 2018; 122(8):1303-1309. Annals of Emergency Medicine 2012;60:45-56. In summary: At a cutpoint of 17.0, it is 97% sensitive. At a cutpoint of 19.0, it is 97% specific.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content