This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
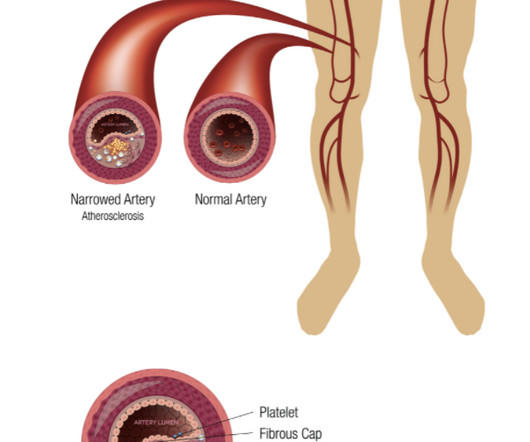
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
Diseased human arteries are most simply, reliably, and successfully treated with drug-eluting, balloon-expandable stents," said Lewis B. 2 An estimated 10% of patients with PAOD have its most severe form: chronic limb-threatening ischemia (CLTI). Eur J Vasc Endovasc Surg. 2012;43:55-61. J Am Heart Assoc. DOI: 10.1161/JAHA.118.009724.
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Normal FFR is 1.0 and an FFR below 0.75 in the study.
Method Between June 2018 and December 2022, 62 patients with type A aortic dissection (TAAD) underwent reoperation after previous surgical treatment. Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. The total occlusion was recanalized and stented from 100 to 0%. Clinical: patient alerts for refractory ischemia (refractory chest pain), and empowering nurses to advocate for patients 4. Hyperacute T-waves remain in V3 and V4.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Just before 10 AM, the patient received a stent to the culprit OM. We know that today's patient has had prior inferior OMI with stenting of his proximal RCA ~3 years earlier. Peak troponin was 12 ng/mL.
He did, found the true culprit, and went back in to stent it. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. See P.S. below ) == P.S. : I believe I found another example of ischemia-induced J waves ( See Oct.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. A mid-LAD culprit lesion was identified and stented. Pacing Clin Electrophysiol. 40; 1234-1241.
One stent was deployed with restorative TIMI-0 flow. Accurate identification is absolutely necessary as this pattern can be easily misinterpreted for something less nefarious: for example, generic “subendocardial ischemia.” However, when the Troponin I returned 8.4 The red arrow shows a 90% LAD occlusion at the D1 branch.
He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. It’s important to stress the presence of a normal QRS (i.e., This first image shows turbulent flow through stenotic narrowing of the vessel. Journal of Electrocardiology, 50 , 561-569. 3] Aslanger, E.,
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The lesion was stented. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. Circ Cardiovasc Interv.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. A 99% LAD occlusion was stented. BP 110/67 HR 68 RR 14 (non-labored) SpO2 95 RA Physical exam revealed slight pallor and diaphoresis. Attached is the first ECG. 5] Walsh, B.
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6. Progression of V2 showing posterior involvement.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. The culprit lesion was opened and stented. For more on this mirror-image opposite ST-T wave relation in leads III vs aVL — See My Comment in the March 8, 2019 and August 9, 2018 posts in Dr. Smith's ECG Blog ).
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. In there ECG evidence of possible ongoing ischemia? (ie, THANK YOU Dr. Lee!
This ECG is all but diagnostic of subepicardial ischemia of the anterior, lateral, and inferior walls, most likely due to Occlusion MI (OMI), probably of the LAD. They found an acute lesion of the LAD at the site of the prior stents, including 70% proximal LAD lesion and 95% mid-LAD stenosis with TIMI 3 flow at the time of cath.
It was stented. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. My Comment , by K EN G RAUER, MD ( 10/24/2018 ): = Important teaching points are made in this post by Dr. Smith. Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5,
This is where careful discussion with the patient is required, and an explanation of the most recent literature suggests no reduction in future major heart events with stenting in most obstructive coronary artery disease 5. ( 2018 Sep 6;379(10):924-933. 5 ISCHEMIA Research Group. 5 ISCHEMIA Research Group. N Engl J Med.
So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent. EKG shown here: LAFB with no clear signs of OMI or ischemia. Queen of Hearts interpretation: Now the cardiologist considered it "STEMI"! No labs were performed. EKG and CT head were performed.
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia). The patient recovered well. J Am Heart Assoc.
Am J Cardiol 2018; 122(8):1303-1309. After many hours, the decided that it was appropriate to do an angiogram and they found a distal LAD occlusion which was opened and stented. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. link] Chatzidou, S.,
It was opened and stented. Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The January 30, 2018 post — for PTA.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content