This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
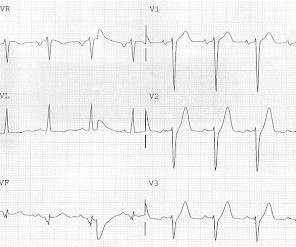
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
mmm ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
European Heart Journal , ehy651, [link] Published: 26 October 2018 [link] Timing of revascularization in patients with transient ST-segment elevation myocardial infarction: a randomized clinical trial. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded.
ECG Blog #193 — Reviews the concept of why the term “OMI” ( = O cclusion-based MI ) should replace the more familiar term STEMI — and — reviews the basics on how to predict the " culprit " artery. The July 31, 2018 post in Dr. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ).
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) I interpret tracings systematically in "real time" ( including my assessment for acute ischemia ).
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
[link] deWinter first reported his unique characteristics of LAD occlusion in 2008, and since the respective ECG changes do not fit the conventional STEMI paradigm (as he even stated – “instead of signature ST-segment elevation” ….) it has been subsequently deemed a STEMI-equivalent.
If it is STEMI, it would have to be RBBB with STEMI. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada.
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. It is often confused with a wide QRS due to conditions such as hyperkalemia. Which artery?
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
This ECG is all but diagnostic of subepicardial ischemia of the anterior, lateral, and inferior walls, most likely due to Occlusion MI (OMI), probably of the LAD. There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. Here is his ECG on arrival: What do you think?
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
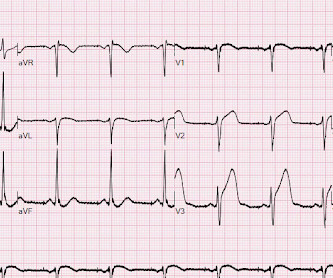
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. Then there is the significant ST elevation we see in lead V1.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion. This was my interpretation: although most ischemic T-wave inversion is post -ischemic like Wellens, sometime active ischemia results in isolated T-wave inversion. We assumed this was Wellens' syndrome and treated as such.
Here is our abstract from SAEM 2018. The MSC were highly sensitive and specific for the diagnosis of ACO in patients presenting to the ED with VPR and symptoms of acute coronary syndrome. == MY Comment , by K EN G RAUER, MD ( 10/3 /2018 ): == How good are paced tracings for detecting ACO ( A cute C oronary O cclusion ) ?
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Chapter 6: Introduction to Myocardial Ischemia and Infarction. Wolters-Kluwer: Philadelphia, PA. [2]
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. A previous ECG from 4 years prior was normal: This looks like an anterior STEMI, but it is complicated by tachycardia (which can greatly elevate ST segments) and by the presentation which is of fever and sepsis.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Of the 418 patient with ACO, 29% did not meet “STEMI criteria.”
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. 72; Issue 9; 2018 ) — A ) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. —
Here is a repeat ECG 45 minutes later with persistent chest pain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3. Repeat ECGs make difficult decisions easier. -- Comment by K EN G RAUER, MD ( 12/29/2018 ): -- Superb case by Dr. Pendell Meyers, which highlights recognition of subtle acute findings.
It is equivalent to a transient STEMI. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. Hayes, S.N.,
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. Angie Lobo ( @aloboMD ) (For open-access reviews of this literature, see Saw 2016 , Saw 2017 , or Hayes 2018.)
Additional Teaching Points: Type-2 MI ( M yocardial I nfarction ) — is defined by an increase in troponin with evidence of ischemia that is not due acute coronary disease, but which instead results from a mismatch in oxygen supply and demand ( Smilowitz et al — Coron Artery Dis 29(1):46-52, 2018 ).
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. 72; Issue 9; 2018.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Am J Cardiol 2018; 122(8):1303-1309. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. It’s important to stress the presence of a normal QRS (i.e., 3] Aslanger, E.,
Learning Points: Atrial flutter can be very tricky to identify, and can cause all kinds of problems such as mimicking or concealing ischemia and OMI. Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Her rate control regimen was stabilized on carvedilol and diltiazem. She was discharged home.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. In this context, patient pain free — post-PCI and with the previous ECGs in mind— the large inferior T waves represent reciprocal change from lateral reperfusion T waves and are not hyperacute T waves of ischemia.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). In there ECG evidence of possible ongoing ischemia? (ie, IMPRESSION: I’d interpret this tracing as consistent with LVH and/or “strain” and/or ischemia. THANK YOU Dr. Lee!
I know from reading your blog that you "diagnose pericarditis at your own peril", but are there any signs on that initial ECG that would make you think ischemia? Journal of Electrocardiology 2018. See this case: Pericarditis, or Anterior STEMI? "TnI peaked at 67.10 ng/mL post PCI." "I 0 0 1 24 140 MMRF 1 1 163 14.0
They recorded a prehospital ECG and diagnosed STEMI and activated the cath lab prehospital. This ST-T wave appearance in the lateral chest leads of ECG #2 is consistent with L V “ S train” vs ischemia. When medics arrived, he denied any chest pain, shortness of breath, or palpitations prior to the syncopal episode.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
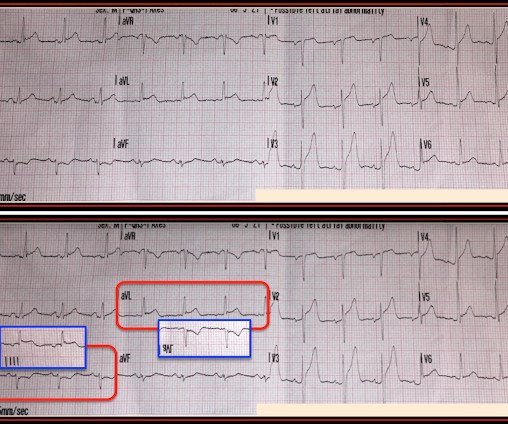
These findings are concerning for inferior wall ischemia with possible posterior wall involvement. The morphology in V2 is also concerning and it appears that the ST segment is being pushed down, as in ST depression. In lead III there is the tiniest possible amount of STE which is difficult to measure due to the very low-voltage.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content