This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
See these 2 articles Association between pre-hospital chest pain severity and myocardial injury in ST elevation myocardialinfarction: A post-hoc analysis of the AVOID study Author links open overlay panel [link] 1 Background We sought to determine if an association exists between prehospital chest pain severity and markers of myocardial injury.
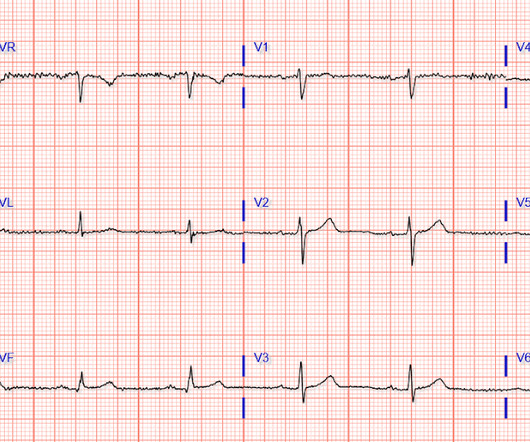
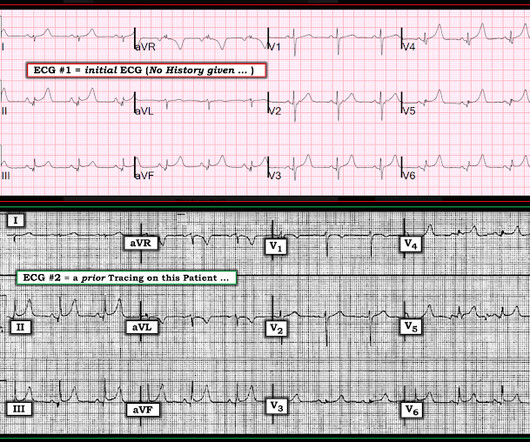
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. What do you think?
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely. NTG drip started.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Comparative early and late outcomes after primary percutaneous coronary intervention in st-segment elevation and Non–St-segment elevation acute myocardialinfarction (from the Cadillac trial). & Griffin, J. link] Lee, T. Weisberg, M.,
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. The “bottom line” conclusions of their case report were that transient J waves may on occasion be induced by an acute injury current from impending myocardialinfarction.
This is diagnostic of myocardialinfarction. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
Although not striking, this is clearly a diagnostic ECG for infero"posterior" myocardialinfarction due to coronary occlusion (OMI), most likely due to left circumflex (LCx) artery occlusion. mm STE even in the fourth universal definition of myocardialinfarction. Considerations on the naming of myocardialinfarctions.
This confirms that there were dynamic signs of ischemia on the initial ECG. ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. The ST depression in aVL is also resolved. It was not normal! A third troponin I returned at 0.27
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. There is also a Q-wave in III. There is also subtle STD in V3-V5. The initial troponin I was elevated at 0.75
Electrocardiographic differentiation of early repolarization from subtle anterior ST-segment elevation myocardialinfarction. It’s important to stress the presence of a normal QRS (i.e., With deliberate practice, spot diagnosis of T-to-R ratio will come with time. References 1] Smith, S. Annals of Emergency Medicine, 60 (1), 45-56.
Here it is: Computer Interpretation: SINUS RHYTHM INFERIOR MYOCARDIALINFARCTION, POSSIBLY ACUTE ST ELEVATION, CONSIDER ANTERIOR INJURY [MARKED ST ELEVATION W/O NORMALLY INFLECTED T WAVE IN V2-V5] ACUTE MI What do you think? This ECG was texted to me with no information: I answered: "Show me the whole 12-lead."
He was found diaphoretic and uncomfortable, and verbalizing a prior history of myocardialinfarction and that, furthermore, the acute symptoms were identical to that which had been associated with RCA stent placement 4 years prior. Terminal QRS distortion is present in anterior myocardialinfarction but absent in early repolarization.
Diagnostic and prognostic value of the QRS-T-angle, an ECG marker quantifying heterogeneity of depolarization and repolarization, in patients with suspected non-ST-elevation myocardial infarc tion. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6.
If the patient had been "lucky," his symptoms from the prior day might have been due to ischemia prolonged and intense enough to result in small troponin increase. Diagnosis of acute myocardialinfarction in angiographically documented occluded infarct vessel: limitations of ST-segment elevation in standard and extended ECG leads.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. Am J Cardiol 2018; 122(8):1303-1309. To me, this makes the ECG nearly diagnostic of ischemia, though if it is LAD occlusion, there should be ST depression in III and aVL, so it is a bit confusing.
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. Utilization of coronary computed tomography angiography and computed tomography-derived fractional flow reserve in a critical limb-threatening ischemia cohort.”
In some cases the ischemia can be seen "through" the flutter waves, whereas in other cases the arrhythmia must be terminated before the ischemia can be clearly distinguished. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia.
His father and brother both died of myocardialinfarction at ages 61 and 45, respectively. There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1]
indicates inducible ischemia while an FFR above 0.80 excludes ischemia in 90% of cases. They had lower rates of mortality or myocardialinfarction. myocardialinfarction rate and 3.2% There is a strong correlation between FFR and inducible myocardialischemia. Normal FFR is 1.0 An FFR below 0.75
The primary endpoint of this study was major adverse cardiovascular and cerebrovascular events (MACCEs) that included all-cause mortality, non-fatal myocardialinfarction, non-fatal ischemic stroke, and ischemia-driven revascularization.Results:The average age of the study participants was 59.55 ± 10.98
Diagnosis of Acute MyocardialInfarction in the Presence of Left Bundle Branch Block using the ST Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Electrocardiographic Diagnosis of Acute Coronary Occlusion MyocardialInfarction in Ventricular Paced Rhythm Using the Modified Sgarbossa Criteria.
European Heart Journal , ehy651, [link] Published: 26 October 2018 [link] Timing of revascularization in patients with transient ST-segment elevation myocardialinfarction: a randomized clinical trial. MRI measure infarct size was the same in both. All patients received aspirin, a P2Y12 inhibitor, and an anticoagulant.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). Acute myocardialinfarction in patients with dialysis Patients on dialysis have a well studied history of underdiagnosis and undertreatment for acute myocardialinfarction.
Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Published 2018 Feb 6. Efficacy and Safety of Low-Dose Colchicine after MyocardialInfarction. 4 In the U.S. 12 Colchicine, 0.5
Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chest pain for the ischemia and potential syncope for brugada. Ischemia/infarction. It helps a little bit.
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Impact of total occlusion of culprit artery in acute non-ST elevation myocardialinfarction: a systematic review and meta-analys is.
2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. 2018 Sep 6;379(10):924-933. 5 ISCHEMIA Research Group. 5 ISCHEMIA Research Group. Medicine (Baltimore). 2022 Sep 16;101(37):e30583. N Engl J Med. 3 ESC Scientific Document Group. Eur Heart J. 2020 Jan 14;41(3):407-477. Eur Heart J. N Engl J Med.
In most cases, rather, the culprit is gross ischemia due to myocardialinfarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, today’s case is lacking any such diagnostics, thus I cannot say with certainty that the QT interval is, or is not, culpable in arrhythmogenesis. [1] 6] Goldberger, A.
Compared to TTE from 7/3/24: the anterior regional wall motion abnormality is new and is consistent with ischemia/infarction in the LAD territory == MY Comment , by K EN G RAUER, MD ( 11/20 /2024 ): == There are several insightful aspects of today's case. The January 30, 2018 post — for PTA.
It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Due to the atypical and vague symptoms, the myocardialinfarct was not initially diagnosed. At presentation he had a history of dyspnea for 6 days.
It is possible there is microvascular dysfunction producing residual transmural ischemia. But this is most common when there is prolonged ischemia, and this patient had the fastest reperfusion imaginable! Acute myocardialinfarction: an uncommon complication of takotsubo cardiomyopathy. SanzRuiz, R., Solis, J., &
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content