This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
BackgroundLittle is known about treatment variability across US hospitals for patients with chronic limb‐threatening ischemia (CLTI).Methods Methods and ResultsData were collected from the 2016 to 2018 National Inpatient Sample. Journal of the American Heart Association, Ahead of Print.
The ECG does not show any definite signs of ischemia. Uncontrolled coronary spasm may be associated with serious arrhythmias , including cardiac arrest ( Looi et al — Postgrad Med, 2012 ; Tan et al — Eur Heart J Case Rep, 2018 ; Chevalier et al — JACC, 1998 ; Rodriguez-Manero — EP Europace, 2018 ). The below ECG was recorded.
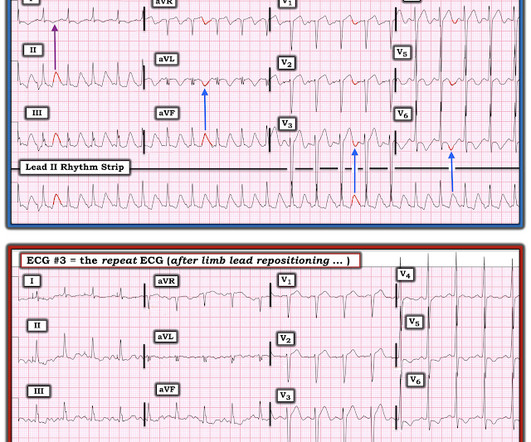
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM LINE: ECG changes of LV "strain" and/or ischemia that we see on today's initial ECG — were not present 9 years earlier. ECG Blog #73 — Reviews "My Take" on the ECG Diagnosis of LVH.
ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ). ECG Blog #271 — Reviews determination of the ST segment baseline ( with discussion of the entity of diffuse Subendocardial Ischemia).
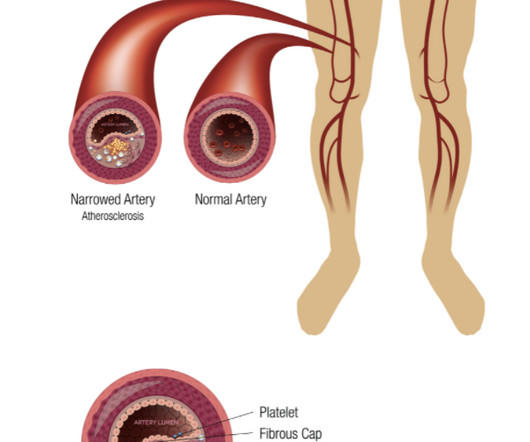
2 An estimated 10% of patients with PAOD have its most severe form: chronic limb-threatening ischemia (CLTI). Determinants of long-term outcomes and costs in the management of critical limb ischemia: A population-based cohort study. Eur J Vasc Endovasc Surg. 2012;43:55-61. J Am Heart Assoc. DOI: 10.1161/JAHA.118.009724. 118.009724.
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. As suggested by Figure-4 below in the ADDENDUM — assessment of the ST-T waves in leads V2,V3 and V5,V6 — is consistent with ischemia and / or LV "strain".
ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS. In the ECG above there are several features indicative of ongoing transmural ischemia. What do you think?
In the days before I learned to look for OMI, back when I was counting ST elevation boxes, I used to save ischemia for last.) In the 500+ Comments I have written on Dr. Smith's ECG Blog since becoming an Associate Editor in 2018 — I do not believe we have had a case of RA-LL lead reversal. The July 29, 2018 post ( LA-RA reversal ).
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The ECG only tells you there is ischemia, not the etiology of it. Nevertheless, the clinical situation made other etiologies unlikely.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
ACUTE MI (I allowed Acute MI to be in the report because I knew there would be an elevated troponin from ischemia, which is the definition of acute MI -- but in this case it would most likely be a Type 2 MI from tachycardia) There is also LA-RA lead reversal. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ).
His response: “subendocardial ischemia. Smith : It should be noted that, in subendocardial ischemia, in contrast to OMI, absence of wall motion abnormality is common. With the history of Afib, CTA abdomen was ordered to r/o mesenteric ischemia vs ischemic colitis vs small bowel obstruction. Anything more on history?
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. In subendocardial ischemia, cath lab is indicated if the pain persists in spite of medical therapy (aspirin, anticoagulant, IV nitro). At 100 minutes, the above ECG was recorded.
But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. But clearly this 'Non-STEMI' patient with OMI would have benefited from immediate cath lab activation on arrival, when their first troponin was 11ng/L, rather than after after it rose to 12,000ng/L after 12 hours of refractory ischemia.
5] Back to the case The patient had serial ECGs over the next hour with no significant change: The first troponin came back at 1,400 ng/L (normal <26 in males and <16 in females), confirming MI – and the patient’s refractory ischemia indicated this was an Occlusion MI.
So, we desperately required to break this inappropriate menace with evidence base like COURAGE, ISCHEMIA, BARI-2D, These studies tried to apply some breaks, but the force was weak and couldn’t abolish a pseudo-academic vice. Something happened in 2018 , the ORBITA trial.It sent real shock waves to the Interventional community.
Chest Pain Severity Rating Is a Poor Predictive Tool in the Diagnosis of ST-Segment Elevation Myocardial Infarction [link] Abstract Current ST-segment elevation myocardial infarction (STEMI) guidelines require persistent electrocardiogram ST-segment elevation, cardiac enzyme changes, and symptoms of myocardial ischemia.
This was my interpretation: although most ischemic T-wave inversion is post -ischemic like Wellens, sometime active ischemia results in isolated T-wave inversion. In such cases, if there is no infarction (necrosis), when the ischemia resolves, the T-wave may normalize (in contrast to Pseudo-normalize).
Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. In view of the lack of J waves in the pre-hospital tracing — it would certainly seen that these J waves were ischemia-induced , and markers of the “culprit artery”.
Objective:Forward head posturing (FHP) has been associated with chronic anatomic vertebral artery disturbances possibly leading to posterior circulation ischemia. Stroke, Volume 55, Issue Suppl_1 , Page ATP252-ATP252, February 1, 2024. The data supporting FHP as a true risk factor of posterior circulation stroke has not been well established.
However, its utilization in the pediatric/young adult population is not well characterized.Methods:We queried the RAPID Insights database from 10/05/2018-09/29/2023 for unique patients between 2-25 years with a CTP.
Our chief of cardiology, Gautam Shroff, interprets it differently and thinks this is indeed ischemia. She was taken to the cath lab and her coronaries were clean!! There was no MRI, but the presumptive diagnosis is myocarditis. I have seen this pattern in severe acute AI also." Smith — this case was not what I thought.
The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Chest trauma was suspected on initial exam. Here is his initial ECG around 1330: What do you think?
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. Neth Heart J 2018. Patel et al.
There is broad subendocardial ischemia as demonstrated by STE aVR with concomitant STD that almost appears appropriately maximal in Leads II and V5. There is LBBB-like morphology with persistent patterns of subendocardial ischemia. This is the initial ECG: The QRS is widened with a regular cadence, and there are no discernable P waves.
The pain will resolve and you will think the ischemia is gone when it is only hidden ! Smith comment: this troponin alone should be enough data to activate the cath lab, regardless of the ECG. Also: As we always say, do not give morphine until you are committed to the cath lab.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. What does this troponin level mean? 2012;5:134–137.
The PEARL is that recognition of a longer-than-expected P wave in a supraventricular tachycardia should bring to mind the “Bix Rule” ( See My Comment at the bottom of the page in the August 3, 2018 post in Dr. Smith's ECG Blog ). Would you give lytics? Yes, but not because of the ECG! Arrhythmia? Electricity, drugs, lytics, cath lab?
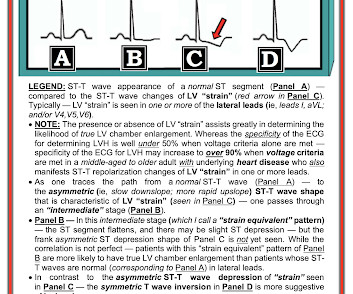
The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. Voltage for LVH ( the R wave in lead aVL easily surpassing 12 mm ).
Additional Teaching Points: Type-2 MI ( M yocardial I nfarction ) — is defined by an increase in troponin with evidence of ischemia that is not due acute coronary disease, but which instead results from a mismatch in oxygen supply and demand ( Smilowitz et al — Coron Artery Dis 29(1):46-52, 2018 ).
The T-waves of both of these beats have, coincidentally , a superimposed P-wave Clinical course: The potassium was normal, there was no ischemia or drug toxicity. Treat ischemia (Cath lab) 3. These are beats in which the pacer captured. She went for emergent pacemaker revision. Treat hyperkalemia or drug toxicity 2. External pacing 5.
Incredibly , this case was just published in Circulation on January 22, 2018 (thanks to Brooks Walsh for finding this!) 2018; 137: 402-404. Originally published January 22, 2018 Here is a case from Circulation year 2000 that was misdiagnosed as due to pancreatitis. Journal of Electrocardiology. 2012;45(1):15-17. 2010.12.162.
Repeat ECGs make difficult decisions easier. -- Comment by K EN G RAUER, MD ( 12/29/2018 ): -- Superb case by Dr. Pendell Meyers, which highlights recognition of subtle acute findings. Although I arrived at the same conclusion as Drs.
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. There is also a Q-wave in III. There is also subtle STD in V3-V5. The initial troponin I was elevated at 0.75
This confirms that there were dynamic signs of ischemia on the initial ECG. Here are many other cases in which the computer algorithm called the ECG completely normal when it was in fact dangerously abnormal. -- Comment by K EN G RAUER, MD ( 12/19/2018 ): -- Illustrative case by Dr. Brooks Walsh regarding a number of important concepts!
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. These include rate-slowing medication recent ischemia/infarction hypothyroidism sleep apnea. This may be another reason for pacer implantation.
This ST-T wave appearance in the lateral chest leads of ECG #2 is consistent with L V “ S train” vs ischemia. The complete lack of chest pain in the history in this patient who has longstanding hypertension strongly suggests that rather than ischemia, this symmetric T wave inversion reflects LV “strain” from marked LVH.
In other words, the inferior ST segments in the first ECG show more straightening which is more concerning for ischemia. In this context, patient pain free — post-PCI and with the previous ECGs in mind— the large inferior T waves represent reciprocal change from lateral reperfusion T waves and are not hyperacute T waves of ischemia.
Learning Points: Atrial flutter can be very tricky to identify, and can cause all kinds of problems such as mimicking or concealing ischemia and OMI. The March 20, 2018 post on Dr. Smith’s ECG Blog illustrates application of a Lewis Lead in a patient in a regular SVT rhythm. She was discharged home.
I know from reading your blog that you "diagnose pericarditis at your own peril", but are there any signs on that initial ECG that would make you think ischemia? Journal of Electrocardiology 2018. "TnI peaked at 67.10 ng/mL post PCI." "I No PR depression, no Spodicks sign, but concave segments which are diffusely elevated.
But when the clinical presentation is sepsis, one must entertain the possibility that the ST elevation is due to demand ischemia, or some other process, and exacerbated by tachycardia. CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
It’s important to stress the presence of a normal QRS (i.e., A new 4-variable formula to differentiate normal variant ST-segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion – adding QRS amplitude of V2 improves the model. Journal of Electrocardiology, 50 , 561-569. 3] Aslanger, E.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content