This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. There is sinus tachycardia. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Sinus tachycardia, which exaggerates ST segments and implies that there is another pathology.
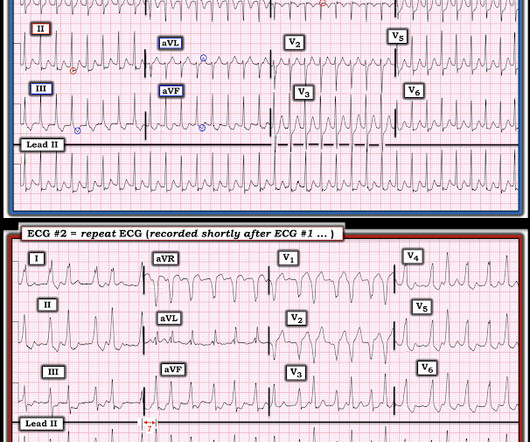
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". He mentioned "cancer" and "chest". There is a narrow complex tachycardia at a rate of 130. He was awake, with a pulse of 130 and BP of 50/30. Is is sinus?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. Sinus Tachycardia and RAD — as already noted above. PEARL # 2: In the absence of associated heart failure ( cardiogenic shock ) — sinus tachycardia is not a common finding in acute MI.
A 30-something presented with chestpain, palpitations, and SOB. The two ECGs above were texted to me with the text: "Young Guy came in in SVT but now in and out of irregular wide complex tachycardia. -- not sure if polymorphic VT vs. a fib with WPW." He has had similar symptoms for 4 years, but has never been evaluated.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? He was intubated for altered mental status.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. If a patient presents with chestpain and a normal heart rate, or with shockable cardiac arrest, then ischemic appearing ST elevation is STEMI until proven otherwise.
This is the prehospital ECG from an 81 year old man with acute chestpain. The problem is, that the PR interval of the upright deflection in lead II ( under the RED arrows ) is relatively long ( clearly more than 1 large box in duration ) — and if anything, the PR interval should shorten when there is tachycardia. Arrhythmia?
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? Troponins 34>33>43, likely secondary to myocardial injury from tachycardia. Sinus tachycardia does not go this fast. A 60-something ow healthy male had syncope while on treadmill. What do you want to do?
Tachycardia (or nearly) 2. And some similar ECGs from Pulmonary Embolism: A young woman with altered mental status and hypotension An elderly woman transferred to you for chestpain, shortness of breath, and positive troponin - does she need the cath lab now? Tachycardia, = 1.8. Poor R-wave progression 4.
Anatomy of a Missed LAD Occlusion (classified as a NonSTEMI) See these examples of Septal STEMI: A man in his 50s with "gas pain" A woman in her 70s with chestpainChestPain and RBBB. Chestpain in a patient with previous inferior STEMI. This is sinus tachycardia at a Rate of ~115/minute.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ).
Given the rapid rate of the tachycardia and the amorphous shape of the QRS — the decision was made to sedate the patient and cardiovert. This phenomenon may sometimes be seen following an episode of a sustained tachycardia — in which marked ST-T wave abnormalities not due to infarction may be seen for a period of hours, or even days!
ie, with syncope-presyncope, fatigue, dyspnea, chestpain? ). 2 short runs of SVT ( presumably atrial tachycardia ). 2 short runs of SVT ( presumably atrial tachycardia ). Checking the rest of the Holter to see if episodes of bradycardia primarily occur at night? Bradycardia was not limited to nighttime hours.
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of ChestPain and Dyspnea Head On Motor Vehicle Collision. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma?
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Read this post: Idiopathic Ventricular Tachycardias for the EM Physician 2. Ken notes AV dissociation.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. We can see enough to make out that the rhythm is sinus tachycardia. The January 30, 2018 post — for PTA.
She denied chestpain and denied feeling any palpitations, even during her triage ECG: What do you think? She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness.
Written by Willy Frick A 57 year old man with was admitted to the hospital with chestpain. The team immediately paged cardiology, concerned for polymorphic ventricular tachycardia. Since sinus conducted QRS complexes cannot co-exist together with ventricular tachycardia, this must all be artifact.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The history in today's case with sudden loss of consciousness followed by chestpain is very suggestive of ACS and type I ischemia as the cause of the ECG changes. What do you think?
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. He complained of generalized weakness and left lower extremity numbness. What is it?
Prior ECG on file: Sinus tachycardia, imperfect baseline, otherwise unremarkable. Triage ECG, with patient awake and complaining of right lower extremity pain: What do you see? Given the absence of chestpain — cardiac contusion is also unlikely. Acute coronary syndrome is unlikely to be one of those entities.
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. It was from a patient with chestpain: Note the obvious Brugada pattern. A rectal temperature was obtained which read 107.9 This patient ruled out for MI.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Heart Rhythm 2018. Her temperature was 106 degrees. Hyperkalemia 2.
A middle-age woman with no previous cardiac history called 911 for chestpain. Methods: Adult, non-traumatic OHCA patients in the ESO Data Collaborative 2018-2023 datasets who experienced OHCA prior to EMS arrival, presented with a shockable rhythm, and received amiodarone or lidocaine during resuscitation were evaluated for inclusion.
A 50-something male presented to triage with chestpain for one day. A Chest X-ray showed infiltrates. Thus, another etiology of chestpain is found, and the fever suggests "fever-induced Brugada." The presenting complaint noted at Triage was, "a 50yo man with chestpain!" The temperature was 39.5
He had no chestpain, dyspnea, or any other anginal equivalent, and his vital signs were normal. This was overtaken by a predominance of sympathetic surge ( tachycardia, persistent ST elevation development of electrical "storm" with failure to respond to recurrent defibrillation ). Circulation Research , 114 (12), 18521866.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content