This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something man presented in shock with severe chestpain. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ).
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
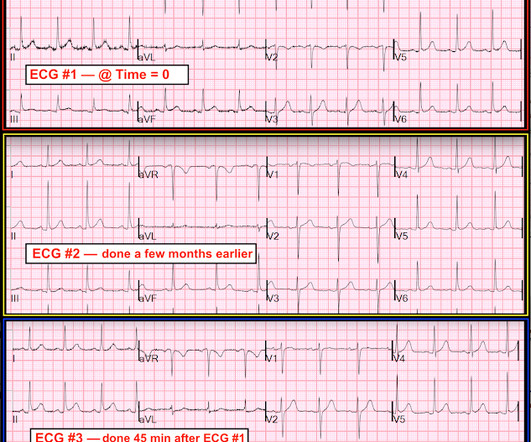
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Echo showed new anterior regional wall motion abnormality and decrease EF from 60% to 45%.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
Angiogram showed a distal RCA occlusion which was stented. While the cath lab was getting ready, we recorded a right sided ECG: V1=V1R which is the same location as V2 V2 = V2R = same location as V1 V3-V6 = V3R - V6R Inferior MI is obvious There is no right ventricular MI evident on these ECGs. Echo showed inferior wall motion abnormality.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion. What do you think? Troponin I peaked at 18.323ng/L.
This patient had the onset of chestpain 24 hours before arrival to the ED. The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. mV compared to 0.05-0.1
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. The patient was found to have total "mid" LAD occlusion which was stented: Pre-PCI. Both were awake and alert with normal vital signs. What do you think? The cath lab was now activated. Smith's ECG Blog ).
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
Am J Cardiol 2018; 122(8):1303-1309. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 QRS V2 = 15.5
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
A 40-something woman had sudden chestpain. He did, found the true culprit, and went back in to stent it. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. She called 911. Learning Points: 1.
The lesion was stented. See this post: Classic Evolution of Wellens' T-waves over 26 hours This is one patient, with ECG recorded at time zero after pain resolution, then at time 2 hours, then at time 9 hours. It seems that there was some uncertainly about this. Circ Cardiovasc Interv. 2012;5:134–137. doi: 10.1161/ CIRCINTERVENTIONS.111.966630.
Factors consistently manifesting as such, in addition to chestpain, include, diaphoresis, vomiting, radiation of pain (most alarming when inclusive of both arms), and pain aggravated by exertion. [1] Troponin I returned 80 ng/mL, and the Cath Lab was then reactivated where a 100% LAD occlusion was found and stented.
The patient contacted EMS after a few hours of chestpain that started 5:30 AM. The pain was described as 6/10 radiating to the right shoulder. The chestpain was described as both sharp and pressure like. The culprit lesion was opened and stented. He is otherwise healthy.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. A mid-LAD culprit lesion was identified and stented. Below are two examples of this. Type II MI), however decided to pursue coronary angiogram out of an abundance of caution.
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. Despite the clinical stability and decreasing pain, this patient needs an immediate angiogram. Here are his publications.)
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina. All is fixed.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
One of the most common questions I get is, “ Do I need a stent to treat my heart disease?” ” Typically, several of this person’s friends have had stents, so it seems natural to ask. First, we must understand what a stent is and why it is used. The stent ‘unblocks’ it. Flow is restored.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Past medical history includes coronary stenting 17 years prior.
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The LAD lesion was acute and required 3 stents to restore flow. Here is his ECG on arrival: What do you think?
It was stented. My Comment , by K EN G RAUER, MD ( 10/24/2018 ): = Important teaching points are made in this post by Dr. Smith. We have previously discussed this phenomenon ( Please see the P.S. at the bottom of the page in My Comment, from Dr. Smith’s July 11, 2018 blog post ). Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5,
Patient 2 : 55 year old with 5 hours of chestpain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. This was missed by the treating physician, but the chestpain resolved with aspirin. This was STEMI(-)OMI.
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. History of diabetes type II and stent placement in 2018. I’m seeing hyperacute T waves III, aVF, down sloping depression I and aVL. What do you think? I responded: "Definite inferior OMI. And Right Ventricular.
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergency department with 3 days of intermittent chestpain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. So which was the culprit?
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? It was opened and stented. The January 30, 2018 post — for PTA. How do I know?
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all. link] Chatzidou, S.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content