This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
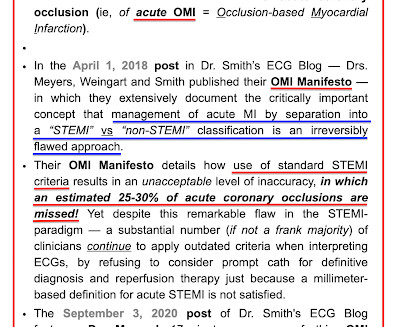
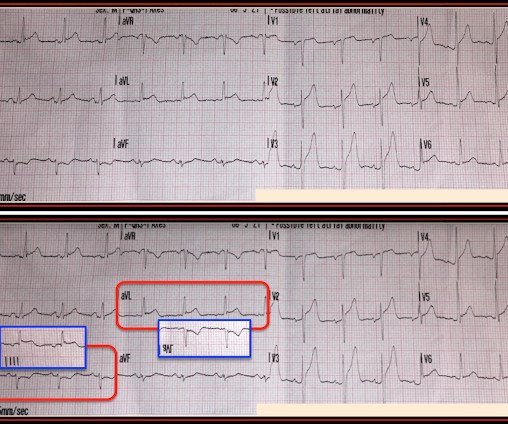
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
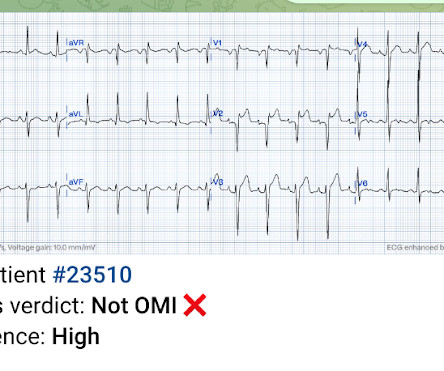
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. What do you think?
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. Chestpain still persists.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD.
A 50-something man presented in shock with severe chestpain. There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch.
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
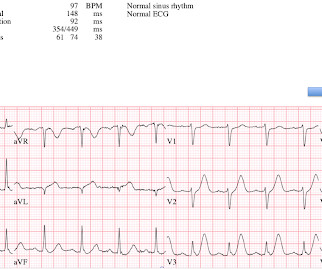
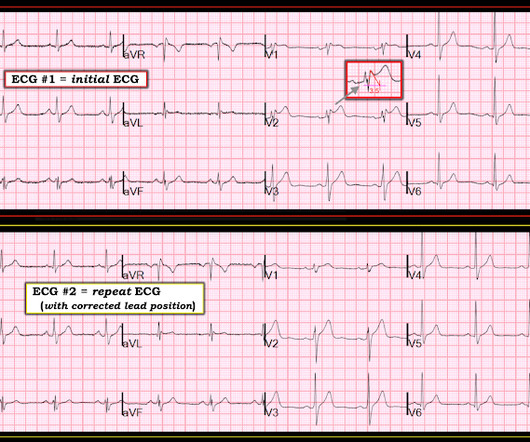
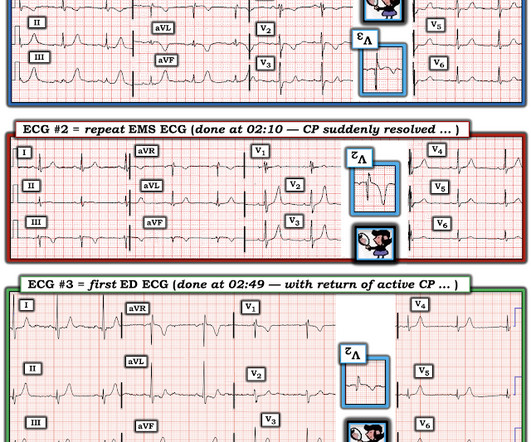
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1. Initial troponin was negative.
The patient presented with chestpain. If it is STEMI, it would have to be RBBB with STEMI. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. This ECG was sent from South Asia.
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. Also ( as per Dr. Smith ) — there is subtle-but-real ST depression in chest leads V2-thru-V5. I was reading ECGs on the system, and saw this one: What do you think?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain!
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
It is from a 50-something with chestpain: What do you think? This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria.
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). The importance of the new OMI ( vs the old STEMI ) Paradigm — See My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Limkakeng AT.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Eur Heart J 2018.
October 2018. link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. Fair enough.
A 50-something presented with epigastric and chestpain. Saddleback ST Elevation is almost never STEMI 2. Here are other cases of saddleback STE: Is this Saddleback a STEMI?? Here is his ECG: What do you think? QTc 388 ms. The patient was diagnosed with reflux Learning Points : 1. wave in V1??
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chestpain that started within the last hour. Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization."
Written by Pendell Meyers A man in his early sixties with no significant medical history (including a "negative cardiac workup a few years ago" for unclear indication) called 911 for acute chestpain constantly for the past 5 hours. However, this patient has active chestpain, and thus this this is inferior-posterior OMI.
Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding. PEARL # 4: When the ECG changes evolve in a way that corresponds to the coming and going of chestpain symptoms — this is important information. BLUE arrows in Figure-2 ).
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
This patient had the onset of chestpain 24 hours before arrival to the ED. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. An ECG was recorded immediately at triage and, at this hospital, the Queen of Hearts is routinely used to determine cath lab activation.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline."
Figure-1: The initial ECG in today's case — obtained from a 50-year old man with new chestpain. ( The deep anterior S waves and tall lateral chest lead R waves suggest significant LVH. The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ). HINT: Is the rhythm sinus ?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria.
The ECG in Figure-1 was obtained from a previously healthy older man — who complained of chestpain and “lightheadedness” while this tracing was recorded. His chestpain had begun the night before. Figure-1: 12-lead ECG and long lead II rhythm strip — obtained from an older man with chestpain and “lightheadedness. (
. = M Y T houghts on the ECG in Figure-1: It's important to remember that the ECG in Figure-1 was obtained from a previously healthy 30-ish year old man who presented with an episode of vasovagal syncope — but there is no mention of chestpain in the history ! B OTTOM L ine : Need for Transfer to a PCI-capable Center?
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Meets formal STEMI criteria in V2-V3.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 1 1/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. My Comment , by K EN G RAUER, MD ( 10/24/2018 ): = Important teaching points are made in this post by Dr. Smith.
The combination of absence of chestpain and history of LV aneurysm made it easy to assess that this patient does not have acute OMI. At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. The patient ruled out by serial troponins.
Steffen writes this case: "A few weeks ago I was able to recognize a STEMI because of what I had seen on your blog." "I I have enclosed the ECG from a 50-something year old male who complained of chestpain. For clarity — I’ve labeled the compressed 12-lead tracing of this 50-ish year old man with new chestpain ( Figure-1 ).
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion. Learning Points: 1.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The day prior to presentation (about 12 hours prior to presentation) he described sudden onset chestpain and shortness of breath while gardening in his back yard. He had no further pain and went to bed that night with no complaints.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Am J Cardiol 2018; 122(8):1303-1309. Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? 100% LAD occlusion.
Denied headache, chestpain, nausea / vomiting. Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 mm in V2 and 4.08
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
A 40-something woman had sudden chestpain. This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI.
Case An elderly patient had acute chestpain and 911 was called. Here is our abstract from SAEM 2018. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think? in leads with at least 1 mm STE.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content