This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
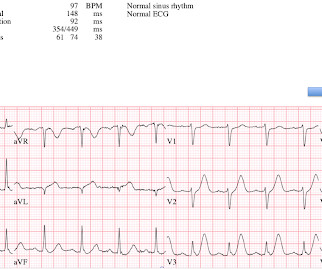
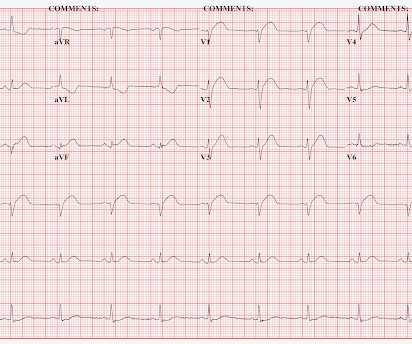
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
A 50-something man presented in shock with severe chestpain. Literature cited In inferior myocardialinfarction, neither ST elevation in lead V1 nor ST depression in lead I are reliable findings for the diagnosis of right ventricular infarction Johanna E. The July 29, 2018 post ( LA-RA reversal ).
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
(Unusual and puzzling, as there was a large focal acute MI) Final Diagnosis: Acute MI, Non ST Elevation MyocardialInfarction. The presence or absence of ST Elevation is a poor marker with which to describe a myocardialinfarction. = NSTEMI is extremely heterogenous, from a very tiny Non-OMI to a massive OMI.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." References Lobo AS et al. JACC 2019 Sep 10;74(10):1290-1300.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardialinfarction. Eur Heart J 2018 4. Who needs the cath lab? Int J Cardiol Heart Vasc 2021 2.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. Eur Heart J 2018. A 70-something y.o. Lemkes et al. Full text link.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Echo showed new anterior regional wall motion abnormality and decrease EF from 60% to 45%. Clin Cardiol 2022 4.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardialinfarctions. On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. She's had multiple PCI procedures.
A middle-aged woman had an acute onset of chestpain and dyspnea. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. It was not normal!
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. EMS gave 324 mg aspirin and 3 sublingual NTG, which the patient stated reduced the substernal chestpain from an 8/10 to 4/10. The ECG only tells you there is ischemia, not the etiology of it.
Here it is: Computer Interpretation: SINUS RHYTHM INFERIOR MYOCARDIALINFARCTION, POSSIBLY ACUTE ST ELEVATION, CONSIDER ANTERIOR INJURY [MARKED ST ELEVATION W/O NORMALLY INFLECTED T WAVE IN V2-V5] ACUTE MI What do you think? If it is a chestpain patient, I would get a formal echo and serial ECGs. And look for an old EKG."
This is obviously diagnostic of inferior and lateral Occlusion MyocardialInfarction. The location of the infarct is clear, but that does not necessarily tell you what artery it is. Electrocardiographic diagnosis of acute coronary Occlusion MyocardialInfarction in ventricular paced rhythm using the modified Sgarbossa criteria.
The finding of dynamic ST-T wave changes on serial tracings in association with a change in chestpain symptoms ( SEE My Comment in the July 21, 2020 post ). Any ST elevation in inferior leads that occurs in association with mirror-image opposite ST depression in lead aVL. ST depression that is maximal in leads V2-to-V4.
This is diagnostic of myocardialinfarction. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. She felt more comfortable being admitted. Int J Cardiol.
A 40-something woman had sudden chestpain. But which myocardial walls are affected? Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. She called 911. Figure-2: TOP — Initial ECG obtained pre-hospital.
Electrocardiographic Differentiation of Early Repolarization FromSubtle Anterior ST-Segment Elevation MyocardialInfarction. Am J Cardiol 2018; 122(8):1303-1309. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5
Case A 39-year-old male without prior medical history presents with chestpain that started 2 hours prior to presentation. He says that the pain intensity was 10/10 at home but now about 4/10. mm STE even in the fourth universal definition of myocardialinfarction. Here are his publications.) What do you think ?
She went on to describe her chestpain as a "buffalo sitting on my chest" and a "weird" sensation in her jaw for 1 hour prior to arrival, associated with lightheadedness and diaphoresis. The patient was given fentanyl initially for chestpain with minimal effect and then vomited which was followed by zofran and famotidine.
We knew only that the ECG belonged to a man in his 50s with chestpain and normal vitals. The day prior to presentation (about 12 hours prior to presentation) he described sudden onset chestpain and shortness of breath while gardening in his back yard. He had no further pain and went to bed that night with no complaints.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Am J Med 2019, 132(5):622-630. Miranda DF, Lobo AS, Walsh B, et al.
The patient had come to the ED for SOB, but without any chestpain. This was not a myocardialinfarction of any kind. Other cases of Pulse Tapping Artifact: Acute chestpain and a bizarre ECG Bizarre (Hyperacute??) Therefore, as many as 11 of the 12 leads can look bizarre. He had a 10 pound weight loss.
Cardiology felt her chestpain to be, most likely, the result of coronary supply-demand mismatch in the context of HCM endothelial remodeling (i.e. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardialinfarction in the emergency department. Below are two examples of this.
Written by Pendell Meyers, with edits by Smith A man in his 80s presented with acute chestpain and normal vital signs. We need more such ECGs for training but we are constantly working on the algorithm and one day it will make this diagnosis. == But isn't ongoing chestpain in NSTEMI a guideline indication for emergent angiography?
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. For more information: www.heartflow.com References 1 Krievins, Dainis K.,
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Why is there this notion that myocardialinfarction cannot be diagnosed in the setting of ventricular paced rhythm?
BACKGROUND:The PRECISE (Prospective Randomized Trial of the Optimal Evaluation of Cardiac Symptoms and Revascularization) demonstrated that a precision diagnostic strategy reduced the primary composite of death, nonfatal myocardialinfarction, or catheterization without obstructive coronary artery disease by 65% in patients with nonacute chestpain (..)
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardialinfarction of any kind.
MI = MyocardialInfarction/Heart Attack However, there are two very important caveats. 2023, 2 Coronary CT Angiography and 5-Year Risk of MyocardialInfarction. 2018 Sep 6;379(10):924-933. So a very low chance. This was compared to using exercise stress testing. Journal of Cardiovascular Computed Tomography, Oct 9.
Background In myocardialinfarction with nonobstructive coronary arteries (MINOCA), there are limited patient-level data on outcomes by sex and race. Methods Patients admitted to a single center with acute myocardialinfarction (MI) between 1 January 2012 and 31 December 2018, were identified by chart and angiographic review.
More than 8 million Americans visit hospital emergency departments experiencing chestpain every year. “In the future, patients with coronary inflammation can be identified by the CaRi-Heart technology and treated by our FDA -approved LODOCO 0.5 mg tablets.” In June 2023, the U.S.
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. Patients on dialysis often do not have chestpain in the setting of acute MI. Why is this?
Background To determine if the European Society of Cardiology 0/1-hour (ESC 0/1-h) algorithm with high-sensitivity cardiac troponin T (hs-cTnT) meets the ≥99% negative predictive value (NPV) safety threshold for 30-day cardiac death or myocardialinfarction (MI) in older, middle-aged and young subgroups.
The utility of the triage electrocardiogram for the detection of ST-segment elevation myocardialinfarction. October 2018. We record ECGs in triage on every patient with chestpain, and some other indications, and this amounts to 8000 ECGs in triage each year, costing at most $200,000 (8000 x $20.00).
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. Mechanical Reperfusion in Patients with Acute MyocardialInfarction Presenting More than 12 Hours from Symptom Onset: A Randomized Controlled Trial. mm STE in V1 and 1.5-2.0
Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. First, the name (MyocardialInfarction or Not) is not important. A subsequent troponin drawn 6 hours after symptom onset , remained below the LoD.
Case An elderly patient had acute chestpain and 911 was called. Details cannot be shared here, but suffice it to say that inability to recognize acute occlusive myocardialinfarction in the presence of ventricular paced rhythm contributed to a poor outcome. Here is our abstract from SAEM 2018. What do you think?
Rachel Bond, MD, FACC, is the system director of the Women's Heart Health Program at Dignity Health in Arizona, which she founded in 2018. That's the only way we can give women a definitive diagnosis for what's causing their chestpain." Acute MyocardialInfarctions in Women. Can J Physiol. 2024;102:431-441.
This was texted to me by a paramedic while I was out running one day: "54 yo male chestpain started at 1pm. History of diabetes type II and stent placement in 2018. Let's see how the PMCardio Queen of Hearts AI Model performs: "Acute Occlusive MyocardialInfarction" She gave this a score of 1.0 (100%
1) Very high initial troponin of 45,000 ng/L 2) A full day of chestpain 3) Q-waves on the ECG, with some T-wave inversion Here is one frame of the CT scan which includes the heart: Can you spot the infarct? The January 30, 2018 post — for PTA. This is then a large MI, but it is subacute. How do I know?
A middle-age woman with no previous cardiac history called 911 for chestpain. Methods: Adult, non-traumatic OHCA patients in the ESO Data Collaborative 2018-2023 datasets who experienced OHCA prior to EMS arrival, presented with a shockable rhythm, and received amiodarone or lidocaine during resuscitation were evaluated for inclusion.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content