This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
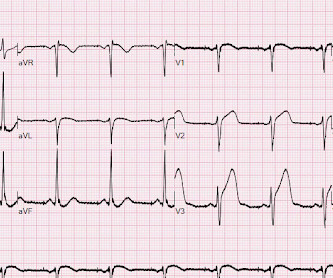
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
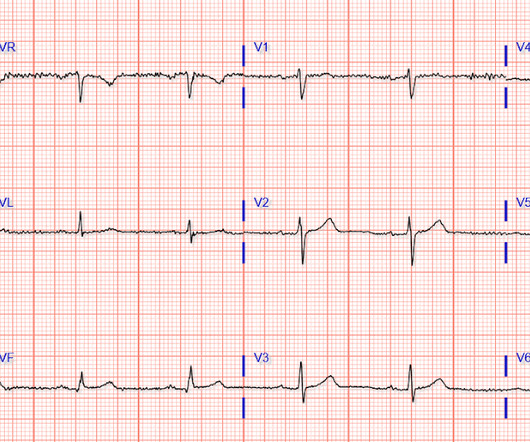
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. The unique " shape " of the prominent ST-T wave abnormalities in this tracing — that are much more suggestive of some significant form of LVH ( L eft V entricular H ypertophy ) rather than ischemia. What do you think now?
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. The ECG does not show any definite signs of ischemia. The below ECG was recorded.
--The STD in V2-V6 might be interpreted as subendocardial ischemia, but with the inferior STE, it is far more likely to represent posterior OMI. Here is the history: A 40-something male had intermittent chest discomfort until 90 minutes prior to presentation, when it became constant. At 100 minutes, the above ECG was recorded.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 2024, [link]. 22, 30 Nov.
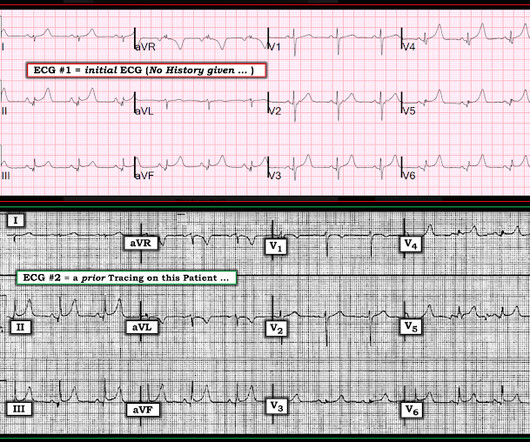
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1. Initial troponin was negative.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This strongly suggests reperfusing RCA ischemia.
The patient presented with chestpain. Followup ECG: No Change Absence of evolution is the best evidence against ischemia as the etiology. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada.
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). ECG Blog #184 — illustrates the "magical" mirror-image opposite relationship with acute ischemia between lead III and lead aVL ( featured in Audio Pearl #2 in this blog post ).
As a result, the ST elevation ( with especially tall, peaked T wave in lead V2) — is not indication of acute ischemia. Today's patient is a middle-aged woman who presented with low back pain, shortness of breath and marked hypertension — but no chestpain.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
My written interpretation on a tracing such as this one would read, "Marked LVH and 'strain' and/or ischemia — with need for clinical correlation." BOTTOM Line: Today's patient presented with a 2-3 day history of chestpain and the ECG shown in Figure-1. ECG Blog #276 — and ECG Blog #309 — Reviews the entity of Giant T waves.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. EKG shown here: LAFB with no clear signs of OMI or ischemia. Triage ECG: What do you think? This is a huge anterolateral OMI.
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. ECG#1 Assessing ischemia on an ECG with wide QRS complexes (AIVR, ventricular pacing, BBB, etc) can be challenging. Many health care providers will simply not attempt to assess ischemia in the presence of a wide QRS.
Subendocardial Ischemia from another Cause ( ie, sustained tachyarrhythmia; cardiac arrest; shock or profound hypotension; GI bleeding; anemia; "sick patient" , etc. ). To EMPHASIZE: This pattern of diffuse Subendocardial Ischemia does not suggest acute coronary occlusion ( ie, it is not the pattern of an acute MI ).
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. But no ECG met STEMI criteria so the patient was referred to cardiology as Non-STEMI.
He woke up alert and with chestpain which he also had experienced intermittently over the previous few days. The first task when assessing a wide complex QRS for ischemia is to identify the end of the QRS. His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started.
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. But it was interpreted as no acute ischemia and the patient was referred to cardiology as Non-STEMI. Cardiology aware.
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chestpain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever.
(In other words, the artery was occluded but has sponteneously reperfused, resulting in pain relief) It is important to monitor patients with Wellens' syndrome for re-occlusion, which is usually, but not always, associated with recurrent chestpain. The patient remained pain free. Learning Points: 1.
When I was shown this ECG, I said it looks like such widespread ischemia that is might be a left main occlusion, or LM ischemia plus circumflex occlusion (high lateral and posterior OMI). Here are some cases of RBBB with LAFB: What is the Diagnosis in this 70-something with ChestPain? There is STE in aVR.
A middle-aged woman had an acute onset of chestpain and dyspnea. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? This confirms that there were dynamic signs of ischemia on the initial ECG. The ST depression in aVL is also resolved.
Traditional methods of non-invasive ischemia testing (stress EKG , stress echo, SPECT , PET , direct-to-cath) can result in false negatives 20-30 percent of the time, which can lead to undetected disease, and false positives over 50 percent of the time, which can lead to unnecessary invasive procedures. Neth Heart J 2018. Patel et al.
Written by Pendell Meyers A male in his 50s with history of HTN, DM, HLD presented with chestpain of less than one hour duration. Here is a repeat ECG 45 minutes later with persistent chestpain: Obviously progressing into a clear STEMI. Here is his triage ECG: What do you think? The ECG was interpreted as non-ischemic.
The best course is to wait until the anatomy is defined by angio, then if proceeding to PCI, add Cangrelor (an IV P2Y12 inhibitor) I sent the ECG and clinical information of a 90-year old with chestpain to Dr. McLaren. His response: “subendocardial ischemia. Anything more on history? J Electrocardiol 2013;46:240-8 2.
This is the prehospital ECG from an 81 year old man with acute chestpain. The PEARL is that recognition of a longer-than-expected P wave in a supraventricular tachycardia should bring to mind the “Bix Rule” ( See My Comment at the bottom of the page in the August 3, 2018 post in Dr. Smith's ECG Blog ). Would you give lytics?
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They opened it.
A 40-something woman had sudden chestpain. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. See P.S. below ) == P.S. : I believe I found another example of ischemia-induced J waves ( See Oct.
Chest trauma was suspected on initial exam. The ECG shows sinus tachycardia with RBBB and LAFB, without clear additional superimposed signs of ischemia. Gunshot wound to the chest with ST Elevation Would your radiologist make this diagnosis, or should you record an ECG in trauma? ST depression. Myocardial Contusion?
No chestpain. Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). Later on during the night of his admission he had a short episode of chestpain that resolved with sublingual nitroglycerin. His vitals were initially normal.
Share ChestPain Symptoms There is no role for CT Calcium Scoring in the setting of someone with chestpain symptoms suspected to be from a narrowed coronary artery. Regardless, if you present with chestpain and get a stress test instead of a CTCA, you are arguably getting an inferior test. I would say yes.
If it is a chestpain patient, I would get a formal echo and serial ECGs. There were no others: Notice the similarities to the ECG above, confirming that they are baseline Then he sent the clinical history, which was of a malfunctioning ICD, but without any chestpain or SOB. And look for an old EKG."
About this time, the 4th troponin, drawn at 8 hours after onset of pain, peaked at 20.956 ng/mL. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. Again, cath lab was not activated. Circ Cardiovasc Interv.
Case An elderly patient had acute chestpain and 911 was called. Here is our abstract from SAEM 2018. And, in cases like the elderly patient with new-onset chestpain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think?
Written by Pendell Meyers, edits by Steve Smith A man in his 60s with history of hypertension and MI 10 years ago, with PCI, presented to an outside hospital complaining of chestpain that started while mowing the lawn. TOP Initial ECG of this 60-year old man with a history of prior MI, who presented with new-onset chestpain.
Am J Cardiol 2018; 122(8):1303-1309. This is the initial ED ECG of a 46 year old male with chestpain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 ng/ml) A 45 year old male called 911 for chestpain: The QTc was 400 ST Elevation at 60 ms after the J-point in lead V3 = 3.5 QRS V2 = 15.5
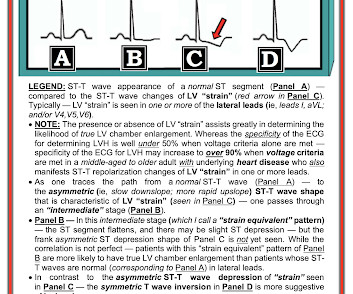
Part of the ST depression with deep T wave inversion in the lateral chest leads clearly reflects LV "strain" from the marked LVH — but despite the very large QRS amplitudes, this ST-T wave appearance looks disproportionate, suggesting at least a component of ischemia. E CG F indings in Today's Tracing N ow M ake S ense !
A 40 something woman with a history of hyperlipidemia and additional risk factors including a smoking history presented with substernal chestpain radiating to "both axilla" as well as the upper back. She was reportedly "pacing in her room while holding her chest". Journal of Electrocardiology 2018. TnI peaked at 67.10
Ischemia Trial In an attempt to clarify this question, a similar trial was done called the Ischemia Trial, which had important differences to the Courage trial but again tried to answer a similar question 3. But what about those with symptoms such as chestpain or shortness of breath as a result of their coronary artery disease?
He denied any chestpain or shortness of breath and stated he felt at his baseline yesterday prior to drug use. They recommended repeating his ECG and awaiting troponin since the patient did not have any chestpain. 72; Issue 9; 2018. He complained of generalized weakness and left lower extremity numbness.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content