This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
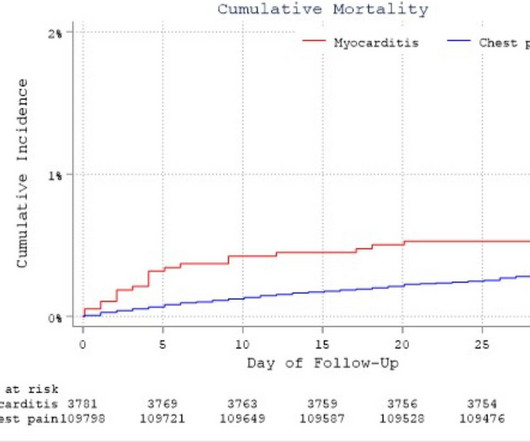
Aims Acute myocarditis (AM) is a disease with variable prognosis, ranging from complete recovery to end-stage heart failure (HF) and death but often challenging to differentiate from unexplained acute chestpain (UCP) in the acute setting. Chestpain was the most common presenting symptom in both groups. 95% CI 1.69
2 middle aged males presented with chestpain. Which had the more severe chestpain at the time of the ECG? Patient 2 at the bottom with a very subtle OMI complained of 10/10 chestpain at the time the ECG was recorded. 414 patients were included in the analysis.
Written by Jesse McLaren A 50 year old presented to triage with one hour of chestpain, and the following ECG labeled normal by the computer (GE Marquette SL) algorithm. What do you think? Theres normal sinus rhythm, first degree AV block, early R wave, normal voltages. Here is her ECG: What do you think?
I went to the patient's chart: Elderly woman with stuttering chestpain and SOB, and dizziness. I was reading ECGs on the system and saw this one, and instantly knew the probable ECG diagnosis: What do you think? What do you think now? This is a very typical ECG for Hypertrophic Cardiomyopathy.
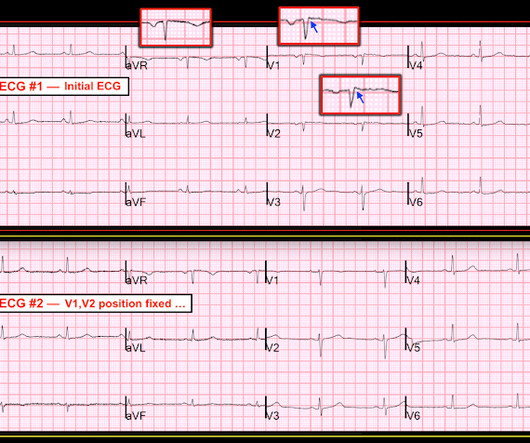
A 50-something man presented in shock with severe chestpain. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ). His prehospital ECG was diagnostic of inferior posterior OMI.
A healthy 45-year-old female presented with chestpain, with normal vitals. The patient was previously healthy, with no atherosclerotic risk factors, and developed chestpain after an episode of stress. The pain was crushing retrosternal, radiated to the arms and was associated with lightheadedness.
Submitted by anonymous, written by Pendell Meyers A woman in her 50s presented to the Emergency Department with chestpain and shortness of breath that woke her from sleep, with diaphoresis. See these other cases of arterial pulse tapping artifact: A 60 year old with chestpain Are these Hyperacute T-waves? 2010.12.162.
A middle-aged patient with lung cancer had presented to clinic complaining of generalized malaise, cough, and chestpain. Symptoms other than chestpain (malaise, cough in a cancer patient) 2. Inclusion criteria were chestpain, at least 2 serial cTnI in 24 hours, sinus rhythm , and at least 1 ECG.
The patient presented due to chestpain that was typical in nature, retrosternal and radiating to the left arm and neck. He denied any exertional chestpain. It is unclear if the patient was pain free at this time. He has a medical hx notable for hypertension, hyperlipidemia and previous tobacco use disorder.
They had difficulty describing their symptoms, but complained of severe weakness, nausea, vomiting, headache, and chestpain. They described the chestpain as severe, crushing, and non-radiating. Altogether, this strongly suggests inferolateral OMI, particularly in a patient with acute chestpain.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." A similar episode had occurred a week earlier during labor.
My Comment by K EN G RAUER, MD ( 2/22 /2023 ): = Today’s case is an important one, because as per Dr. Smith ( in this patient with new chestpain ) — “The initial ECG is diagnostic of infero-postero OMI.” Also ( as per Dr. Smith ) — there is subtle-but-real ST depression in chest leads V2-thru-V5.
A 60 year old with chestpain presented to the ED. In this case, lead I does not look bizarre, but all other leads do. == N OTE : The reasons I especially liked today's case are: i ) The patient presented with chestpain — so the importance of distinguishing artifact from reality can not be overstated! —
The patient presented with chestpain. I was taught that the tell-tale sign of ischemia vs an electrical abnormality was in the hx, i.e. chestpain for the ischemia and potential syncope for brugada. Only 5-18% of ED patients with chestpain have a myocardial infarction of any kind. Is it Brugada pattern?
Case written and submitted by Ryan Barnicle MD, with edits by Pendell Meyers While vacationing on one of the islands off the northeast coast, a healthy 70ish year old male presented to the island health center for an evaluation of chestpain. The chestpain started about one hour prior to arrival while bike riding.
Written by Jesse McLaren Two 70 year olds had acute chestpain with nausea and shortness of breath, and called paramedics. Eur Heart J 2018 4. Today's patient is a 70-year old adult who called EMS because of new-onset chestpain , associated with nausea and shortness of breath. Who needs the cath lab? Lemkes et al.
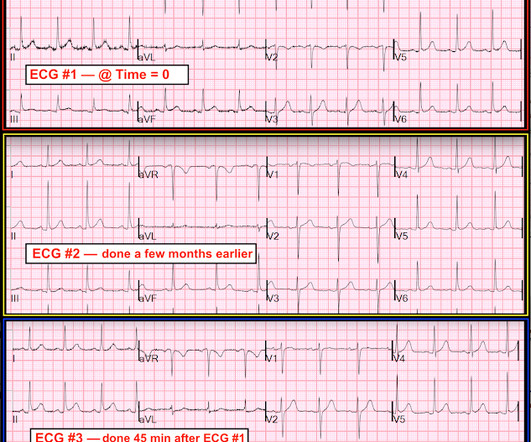
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5.
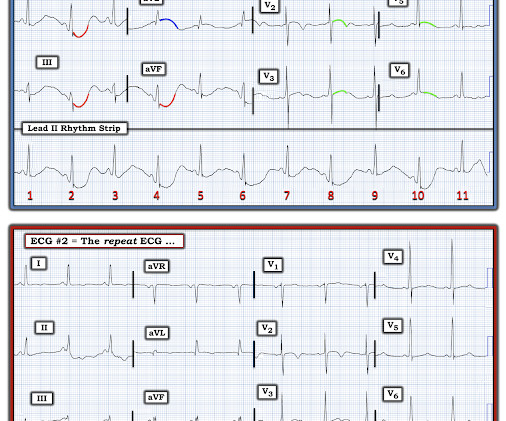
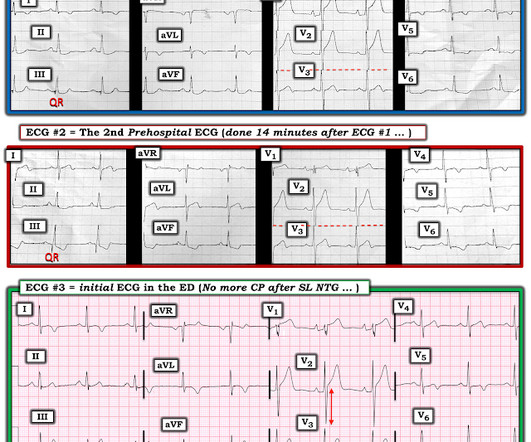
For full discussion of this case — See ECG Blog #292 — == The 2 ECGs shown in Figure-1 were obtained from a man in his 30s — who presented to the ED ( E mergency D epartment ) with chestpain that began several hours earlier. ECG #2 was recorded 1 hour after ECG #1. Initial troponin was negative.
A middle-aged woman presented with chestpain. American Journal of Emergency Medicine 36(5):865-870; May 2018. My Comment, by K EN G RAUER, MD ( 11/4/2018 ): = Important post by Dr. Smith regarding recognition of chest lead misplacement of leads V1 and V2. 27, 2018 blog post ).
It is from a 50-something with chestpain: What do you think? Meyers, Weingart and Smith in their 2018 OMI Manifesto. I like to start my ECG assessment in patients with new chestpain by looking for at least 1 or 2 leads that I know are definitely abnormal. This was sent to me by a friend.
5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chestpain patients. European Journal of Vascular and Endovascular Surgery, vol. 301–302, [link].
BACKGROUND:The PRECISE (Prospective Randomized Trial of the Optimal Evaluation of Cardiac Symptoms and Revascularization) demonstrated that a precision diagnostic strategy reduced the primary composite of death, nonfatal myocardial infarction, or catheterization without obstructive coronary artery disease by 65% in patients with nonacute chestpain (..)
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chestpain onset around 9 PM the evening prior. The following ECG was obtained.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chestpain. Triage ECG: What do you think? This is diagnostic of proximal LAD occlusion. This is a huge anterolateral OMI. I cannot be anything else.
Impression: In this middle-aged man with palpitations and dyspnea, but no chestpain — I suspect that the T wave peaking and slight, upward-sloping chest lead ST elevation represent a repolarization variant. The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ).
After only 90 minutes of chestpain, the first troponin was unsurprisingly in the normal range at 11ng/L (normal <26 in males and <16 in females), so the emergency physician waited for repeat troponin. Chestpain still persists. Paged cardiology 0800: patient complains of chestpain. Cardiology aware.
many readers of this blog). -- Comment by K EN G RAUER, MD ( 9/11/2018 ): -- The lesson in this case relates to the recognition of subtle abnormalities that typically go undetected by the computerized interpretation — and which also may be overlooked by clinicians in the setting of a busy ED.
A 30-something presented with chestpain, palpitations, and SOB. This finding is typical for a post-ablation memory T wave pattern — which is often considered evidence of a successful ablation ( Silverman et al — J Investig Med: Jan, 2018 ). He has had similar symptoms for 4 years, but has never been evaluated.
In the evening, a middle-aged man complained of chestpain at the nursing home. His chestpain was vague. He mentioned "cancer" and "chest". Nurses found him with a BP of 50/30 and heart rate of 130 and called EMS. He was awake, with a pulse of 130 and BP of 50/30. Fluids were started.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Eur Heart J 2018. Wellen's waves indicate that, when the patient was having chestpain, there was occlusion. See these casese (and I have many others): First ED ECG is Wellens' (pain free).
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. Echo showed new anterior regional wall motion abnormality and decrease EF from 60% to 45%.
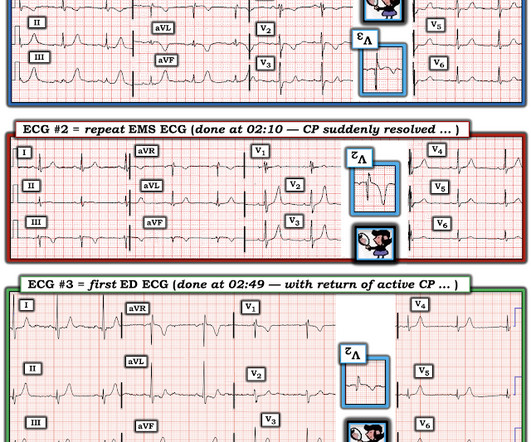
ECG #2 was actually done first, at the time the EMS unit arrived on the scene ( at which time the patient was having severe chestpain ). The July 31, 2018 post in Dr. Smith's ECG Blog ( Please scroll down to the bottom of the page to see My Comment ). Figure-2: Comparison between the 2 ECGs recorded in today's case.
Written by Pendell Meyers A man in his early sixties with no significant medical history (including a "negative cardiac workup a few years ago" for unclear indication) called 911 for acute chestpain constantly for the past 5 hours. However, this patient has active chestpain, and thus this this is inferior-posterior OMI.
He denied chestpain or shortness of breath. In the clinical context of weakness and fever, without chestpain or shortness of breath, the likelihood of Brugada pattern is obviously much higher. Today's patient presented with acute weakness, syncope and fever, but no chestpain or shortness of breath.
This patient had the onset of chestpain 24 hours before arrival to the ED. The above said — in today's patient with a convincing history of chestpain, this initial ECG in Figure-1 was all that was needed for prompt diagnosis of acute postero-lateral OMI. Here is that ECG: Original ECG What do you think?
Today’s patient presented to the ED not only with chestpain — but also with shortness of breath , therefore with a history potentially consistent with the diagnosis. Excellent review of diagnostic testing for acute PE ( Moore et al — Cardiovasc Diagn Ther 8(3):225-243, 2018 ).
October 2018. We record ECGs in triage on every patient with chestpain, and some other indications, and this amounts to 8000 ECGs in triage each year, costing at most $200,000 (8000 x $20.00). A patient with chestpain: See the computer analysis. This paper was just published: Noll S.
Having looked for negative U waves in patients with chestpain over a period of decades — I'll emphasize that this is not a common finding. PEARL # 4: When the ECG changes evolve in a way that corresponds to the coming and going of chestpain symptoms — this is important information. BLUE arrows in Figure-2 ).
For additional examples of this phenomenon whereby automatic truncation of an EMS ECG may mistakenly result in LVH serving to mimi c ischemia — Check out My Comment at the bottom of the page of the following posts in Dr. Smith's ECG Blog — the November 29, 2023 post — June 20, 2020 — March 31, 2019 — March 29, 2019 — and t he December 27, 2018 post.
More than 8 million Americans visit hospital emergency departments experiencing chestpain every year. “In the future, patients with coronary inflammation can be identified by the CaRi-Heart technology and treated by our FDA -approved LODOCO 0.5 mg tablets.”
On the day of presentation she complained of typical chestpain, and stated it feels like prior MI. As I illustrated in detail in My Comment of the October 3, 2018 post of Dr. Smith's ECG Blog — I favor a qualitative approach based on shape. The question is, does she need to go urgently to the cath lab or can she wait.
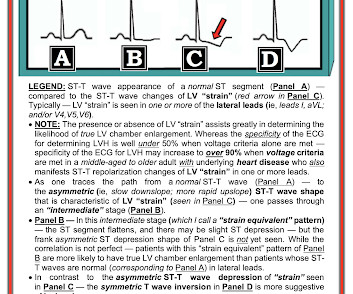
On the other hand — the ST elevation seen in lead V1 is perfectly consistent with LVH and LV "strain" ( ie, The shape of this ST-T wave in lead V1, in association with the deep S wave in this lead — is a mirror-image opposite picture of the typical expected appearance of LVH with "strain" in a lateral chest lead ).
This causes angina, a type of chestpain which is characterized as refractory angina when this pain cannot be controlled by a combination of optimal medical therapy, angioplasty or bypass surgery, and is estimated to impact 600,000 to 1.8 million patients in the United States.
In the last post, we saw how important old ECGs are in assessing the current ECG in a patient without atypical presentation (in this previous case, the patient had no chestpain, and the apparent inferior OMI did not have reciprocal ST depression in lead aVL). She has no chest symptoms. What is the diagnosis?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content