This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In fact, the ECG was described as normal, and without serial ECGs or prior ECGs for comparison it could be. Initial high sensitivity troponin I returned at 6ng/L (normal 0.20 As a result — an ICD may need to be considered in selected cases. Use ß-blockers with caution ( as they may aggravate coronary spasm ).
Her vital signs were within normal limits except for bradycardia at 55 bpm. It is probably sinus bradycardia with very small/depressed P-waves and prolonged PR interval. P EARL # 4 In my opinion, it is not worth wasting time trying to figure out the specific rhythm diagnosis of a bradycardia when there is hyperkalemia.
For instance, if there were inappropriate sinus bradycardia at less than 60 bpm, the atrial pacer would take over if it is programmed to wait 1 second before firing. The atrial lead would pace if, after a programmed period of time, it did not sense an atrial beat (usually 1 second, corresponding to a rate of 60).
The rhythm is sinus bradycardia at a rate just over 50/minute. For review — Check out My Comment — at the bottom of the page in the following posts on Dr. Smith's ECG Blog: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ).
to 1828 msec. ) — which corresponds to a variation in the rate of sinus bradycardia from 36-to-33/minute. This makes sense given that the underlying rhythm in today's case appears to be marked sinus bradycardia and arrhythmia , with a ventricular escape rhythm appearing when the SA node rate drops below 33/minute.
Looking first at the long-lead II rhythm strip — there is significant bradycardia , with a heart R ate just under 40/minute. But the point to emphasize — is that it should only take seconds to recognize that there is bradycardia from significant AV block. = Would you approve her for a nonemergent surgical procedure?
My Comment , by K EN G RAUER, MD ( 7/5/2018 ): This blog post provides an excellent example of how a patient with SSS ( = S ick S inus S yndrome ) may present. during which sinus bradycardia and arrhythmia are seen but not to a degree that produces symptoms. The indication for pacemaker placement with SSS is symptomatic bradycardia.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). RBBB in blunt chest trauma seems to be indicative of several RV injury. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). Sinus Tachycardia ( common in any trauma patient. ).
Hyperkalemia causes peaked T waves and the "killer B's of hyperkalemia", including bradycardia, broad QRS complexes, blocks of the AV node and bundle branches, Brugada morphology, and otherwise bizarre morphology including sine wave. With a twist. Do you recognize this ECG yet? Right Bundle Branch Block with ST Elevation in V1?
Here is his ED ECG: There is bradycardia with a junctional escape. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. For review — GO TO: The June 4, 2018 post ( LA-LL reversal ). The July 29, 2018 post ( LA-RA reversal ). The November 4, 2018 post ( Leads V1,V2 misplacement ).
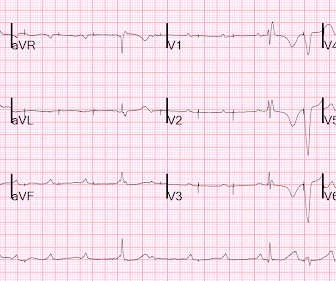
My Thoughts on the Initial ECG: Systematic interpretation of ECG #1 shows: Sinus bradycardia at ~55-60/minute — normal intervals ( PR-QRS-QTc ) — normal frontal plane axis ( about +20 degrees ) — no chamber enlargement. To facilitate comparison in Figure-1 — I put this 2018 prior tracing ( = ECG #3 ) — together with ECG #1.
Athlete’s bradycardia due to increased parasympathetic tone and decreased sympathetic tone is a well-known observation. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described. 2018 Sep;27(9):1052-1062. N Engl J Med.
Hypotension, bradycardia, kidney dysfunction and hyperkalaemia were the main causes of underprescription and/or underdosing, but up to a half of the patients did not receive target doses for unknown causes (51%, 41%, and 55% for BB, ACEi/ARB/ARNI and MRA, respectively). 0.84, and HR 0.74, 95% CI 0.58–0.95, 0.95, respectively).
As per Dr. Nossen — today's initial ECG ( LEFT tracing in Figure-2 ) shows sinus bradycardia with QRS widening due to bifascicular block ( RBBB/LAHB ). There is marked, diffuse ST segment depression in ECG #1.
Am J Cardiol 2018; 122(8):1303-1309. Patient presentation is important This was a 60-something with acute chest pain: There is sinus bradycardia at a rate of 44. In case you were wondering about the T-waves and bradycardia, the K was normal. Why bradycardia? In summary: At a cutpoint of 17.0, it is 97% sensitive.
Hyperkalemia findings include the classic peaked T-waves, as well as the deadly B's of hyperkalemia: Broad (wide QRS), Brady (bradycardia), Blocks (AV blocks), and Bizarre. Learning Points: You must be able to recognize the early stages of hyperkalemia which precede decompensation.
Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018 ). == Distinction is made between 2 types of Brugada ECG patterns: A B rugada - 1 ECG pattern — shows ≥2 mm coved ST elevation with sharp downslope plus T wave inversion in ≥2 anterior leads. Bradycardia. Acute febrile illness. Variations in autonomic tone.
Other Arrhythmias ( PACs, PVCs, AFib, Bradycardia and AV conduction disorders — potentially lethal VT/VFib ). 72; Issue 9; 2018 ) — A ) Brugada-1 ECG pattern, showing coved ST-segment elevation ≥2 mm in ≥1 right precordial lead, followed by a negative T-wave. — Sinus Tachycardia ( common in any trauma patient. ).
Here are inferior leads, and aVL, magnified: A closer inspection of the inferior leads and aVL Sinus bradycardia. J Electrocardiology January–February, 2018; Volume 51, Issue 1, Pages e5–e6. I had no history on the case and no prior ECG for comparison. What do you think?
Because hyperkalemia kills by either VT or VF arrest, or by bradycardia with PEA arrest, this should be assumed to be VT until proven otherwise. In 2018 there is generally a delay to onset of dialysis in most EDs. We set the machine to synchronized cardioversion. We could have also considered terbutaline (start at 0.25
There is sinus bradycardia with one PVC. Shark Fin morphology has been discussed a number of times on Dr. Smith’s ECG Blog ( For review — See the June 11, 2018 post and the January 24, 2020 post , to name just 2 instances ). She then had a 12-lead: What do you think?
Heart Rhythm, 4(2), 198-199. [6] Fever-related arrhythmic events in the multicenter survey on arrhythmic events in Brugada syndrome. Heart Rhythm, 15(9): 1394-1401. [7] 7] American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.
Baseline bradycardia in endurance athletes limits the use of ß-blockers. For more on SSS — See My Comment at the bottom of the page in the July 5, 2018 post in Dr. Smith’s ECG Blog. Clinically — The importance of factoring in increased vagal tone as a contributing factor to AFib episodes — extends into management.
CLICK HERE — for the ESC/ACC/AHA/WHF 2018 Consensus Document on the 4th Universal Definition of MI, in which these concepts are discussed and illustrated.
Additionally, her beta-blocker dose had been decreased because of bradycardia, further predisposing her to atrial flutter. Follow - up: Further discussion with the patient revealed that they had misunderstood the flecainide dosing, and had basically tripled their dose!
To improve visualization — I've digitized the original ECG using PMcardio ) MY Thoughts on the ECG in Figure-1: This is a challenging tracing to interpret — because there is marked bradycardia with an irregular rhythm and a change in QRS morphology. Figure-1: The initial ECG in today's case. ( The QRS complex is wide ( ie, >0.10
We aimed to develop standardized, nationally representative CVD events and selected possible CVD treatment–related complication hospitalization costs for use in cost-effectiveness analyses.METHODS:Nationally representative costs were derived using publicly available inpatient hospital discharge data from the 2012-2018 National Inpatient Sample.
Patient 2 : 55 year old with 5 hours of chest pain radiating to the shoulder, with nausea and shortness of breath ECG: sinus bradycardia, normal conduction, normal axis, normal R wave progression, no hypertrophy. Smith : The fact that the ECG did not evolve is further proof that this was the baseline ECG. nearly identical to the first case).
Regardless of further evaluation, she should avoid bradycardia, AV nodal blockers, Na channel blockers, and fevers. --If Heart Rhythm 2018. --Genetic testing could be helpful to confirm the diagnosis and allow for screening of other at-risk family members. --EP The risk of ventricular fibrillation in asymptomatic patients was 0.9%/y
Within ten minutes, she developed bradycardia, hypotension, and ST changes on monitor. Bradycardia and heart block are very common in RCA OMI. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ). He told the patient this horrible news. link] Chatzidou, S.,
2018 Jan;111(1):59-69. Reference How many of us know there is a journal exclusive dedicated to AF ? Journal of atrial fibrillation 1.Scridon Scridon A, Şerban RC, Chevalier P. Atrial fibrillation: Neurogenic or myogenic? Arch Cardiovasc Dis. doi: 10.1016/j.acvd.2017.11.001. 2017.11.001. Epub 2017 Dec 8. PMID: 29229215. P, Gehi AK.
There are 2 main options: Overdrive pacing could be considered and in the right clinical situation, this is often effective for reducing ventricular arrhythmias ( especially in the case of preventing pause induced or bradycardia-induced arrhythmias in association with QTc prolongation ). Try a different kind of antiarrhythmic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content