This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
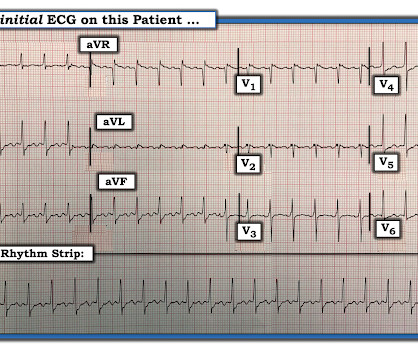
There is a regular wide complex tachycardia. A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. If it is flutter, it will reveal the underlying flutter waves.
Wide-complex tachycardia: VT or aberrant, or "other?" The patient had a history of paroxysmal atrial fibrillation and several cardioversions. A wide-complex tachycardia in an older patient must immediately suggest ventricular tachycardia. Instead, the rate of 150, plus the history of AF, suggested atrialflutter.
This strip was obtained: Apparent Wide Complex Tachycardia at a rate of 280 What do you think? To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex.
There is a narrow complex tachycardia at a rate of 130. ECGs: there is a regular narrow complex tachycardia still at a rate of exactly 130, with no P-waves and also no change since the prehospital ECG. Leads II and aVF appear to have flutter waves. I diagnosed atrialflutter with 2:1 conduction. Is is sinus?
First, we have a narrow-complex, regular tachycardia, with a rate of about 135-140. This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. They are flutter waves, and the rhythm is 2:1 atrialflutter.
There are 2 atrial "bumps" for every QRS. Here I put arrows: Arrows shows slow atrialflutter waves. The PEARL is that recognition of a longer-than-expected P wave in a supraventricular tachycardia should bring to mind the “Bix Rule” ( See My Comment at the bottom of the page in the August 3, 2018 post in Dr. Smith's ECG Blog ).
The principal d ifferential d iagnosis i s similar to what we derived in the October 16, 2019 Case : i ) Sinus Tachycardia ; ii ) Reentry SVT ( either A VNRT if the reentry circuit is contained within the normal AV nodal pathway — or A VRT if an accessory pathway is involved ) ; iii ) AtrialTachycardia ; or iv ) AtrialFlutter.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below. Arch Intern Med.
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter.
Introduction:Supraventricular tachycardia (SVT) is common and poorly tolerated in patients who have undergone Fontan procedure. Rate of recurrence did not differ between those who had the procedure before or after 2018. AtrialTachycardia (70%) and Typical AtrialFlutter (65%) were the most common SVTs ablated.
PurposeAtrial tachycardia is an uncommon supraventricular tachycardia in children. It is often drug-resistant and likely to occur concomitantly with tachycardia-induced cardiomyopathy, making radiofrequency catheter ablation the preferred treatment. A total of 78.6% No postoperative complications occurred in any patient.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content