This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
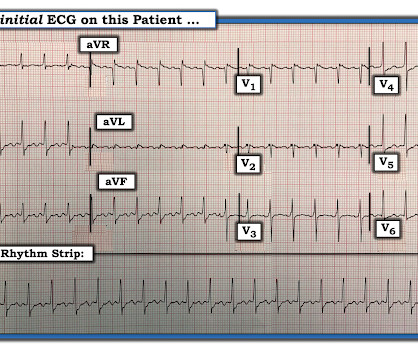
Atrialflutter with 2:1 conduction. The atrialflutter rate is approximately 200 bpm, with 2:1 AV conduction resulting in ventricular rate almost exactly 100 bpm. Further history revealed she had new onset atrialflutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago.
A fully upright P-wave is typical atrial activity of atrialflutter as seen in V1. See these example cases of upright P-waves: Case Continued Thus, I was all but certain that this was atrialflutter. IV Digoxin may begin to slow the ventricular response of AFib or AFlutter sooner than many clinicians realize.
To me, it was clearly atrialflutter with 1:1 conduction. The rate of 280 is just right for atrialflutter. The waves look like atrialflutter waves, NOT like a wide ventricular complex. Reverted to atrial fibrillation with RVR while in the hospital 3 times and needed cardioversion.
The rhythm differential for narrow, regular, and tachycardic is sinus rhythm, SVT (encompassing AVNRT, AVRT, atrial tach, etc), and atrialflutter (another supraventricular rhythm which is usually considered separately from SVTs). Therefore this patient is either in some form of SVT or atrialflutter. If so, why?
This narrows our differential for the rhythm down to sinus tachycardia, paroxysmal supraventricular tachycardia (PSVT, or SVT), and atrialflutter. The patient’s history is notable for paroxysmal atrial fibrillation, which raises clinical suspicion for atrialflutter, since these two entities frequently coexist on a spectrum.
Instead, the rate of 150, plus the history of AF, suggested atrialflutter. A close inspection of lead II showed P or flutter waves at a rate of about 300 bpm, also supporting atrialflutter. There appear to be flutter waves at a rate of 300. Flecainide encourages new atrialflutter.
Rate of recurrence did not differ between those who had the procedure before or after 2018. Atrial Tachycardia (70%) and Typical AtrialFlutter (65%) were the most common SVTs ablated. During the 5-year follow up period, 13 (59%) patients with follow up had cardiovascular (CV) hospitalization and 1 patient died.
There are 2 atrial "bumps" for every QRS. Here I put arrows: Arrows shows slow atrialflutter waves. The PEARL is that recognition of a longer-than-expected P wave in a supraventricular tachycardia should bring to mind the “Bix Rule” ( See My Comment at the bottom of the page in the August 3, 2018 post in Dr. Smith's ECG Blog ).
Re-entrant tachycardias (atrialflutter, PSVT, AVRT, VT) have constant regular heart rates, whereas sinus tachycardia will usually gradually change rate with differing conditions (for instance, after infusion of fluid and BP increase, sinus tach rate might decrease from 130 to 125, for instance). So there is a re-entrant rhythm.
LAFB, atrialflutter, anterolateral STEMI(+) OMI. Fragmentation and artifact ( and possibly already in the inferior leads, the AtrialFlutter pointed out by Dr. Meyers that became obvious in the repeat ECG ) combine to make assessment of ST-T wave changes on many of the leads in ECG #1 difficult.
The principal d ifferential d iagnosis i s similar to what we derived in the October 16, 2019 Case : i ) Sinus Tachycardia ; ii ) Reentry SVT ( either A VNRT if the reentry circuit is contained within the normal AV nodal pathway — or A VRT if an accessory pathway is involved ) ; iii ) Atrial Tachycardia ; or iv ) AtrialFlutter.
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrialflutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway.
of the patients (22/28) who received preoperative pharmacological treatment had intermittent or persistent atrial tachycardia. Of the 28 children who underwent radiofrequency ablation, 24 (85.7%) were diagnosed with focal atrial tachycardia, three (10.7%) with atrialflutter, and one (3.6%) with both. A total of 78.6%
See the September 14, 2018 post for a nice overview of this subject by Dr. Meyers. The differential diagnosis, especially in younger patients, includes atriofascicular tachycardia also known as "Mahaim" tachycardia. The idiopathic VTs are an interesting group of arrhythmias!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content