This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. All of these parameters are important and need to be considered when evaluating plaque regression. REVERSAL Investigators.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. FFR can be useful.
Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
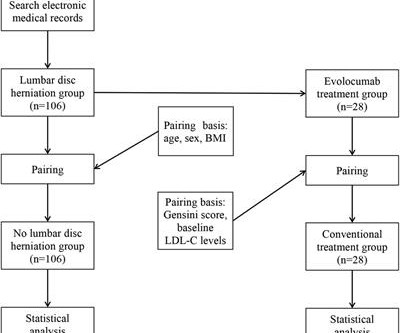
Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective. Methods In this study, a total of 212 patients (age 46–80 years) with unstable angina (UA) who underwent coronary angiography (CAG) in our hospital from January 2018 to July 2022 due to UA were included.
1 Atherosclerosis is a systemic disease that affects multiple vascular regions and is particularly severe in PAD patients, where up to 80 percent suffer from concurrent coronary artery disease (CAD), historically linked with a mortality rate exceeding 50 percent within five years. European Journal of Vascular and Endovascular Surgery, vol.
Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. 2018 Mar;68(668):151-152. 2004 Mar 3;291(9):1071-80. 4 ASTEROID Investigators.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,6 Until recently atherosclerosis has been thought of as the result of passive lipid accumulation in the vessel wall. 4 In the U.S.
BACKGROUND:Sex-specific differences in plaque composition and instability underscore the need to explore circulating markers for better prediction of high-risk plaques. Plaque stability was determined by gold-standard histological classifications. Adipokine, lipid, and immune profiling was conducted.
A CT CAC scan can only identify if there is calcified atherosclerosis, where it is and to what extent. A CTCA provides much more anatomical detail and can identify advanced plaque often missed by CT Coronary Artery Calcium Score scans alone. A CT CAC scan of 0 indicates no significant amount of calcified atherosclerosis.
LDL is obviously a target against atherosclerosis. While the total body seems to do little in determining cholesterol levels, what is more scientifically shocking is slope of the curve between blood LDL levels and plaque burden is rarely linear. 2018 Apr 23;2018:8598054. doi: 10.1155/2018/8598054. 000025% of total fat.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content